Hesam Ahmadi Nooredinvand, Anu Vallipuram, Alice Dawson, Jaymin Patel, Waqar Rashid, Andrew Poullis
{"title":"炎症性肠病临床的半截瘫和半麻醉。","authors":"Hesam Ahmadi Nooredinvand, Anu Vallipuram, Alice Dawson, Jaymin Patel, Waqar Rashid, Andrew Poullis","doi":"10.1177/20542704211035987","DOIUrl":null,"url":null,"abstract":"In this case report, we present a rare case of central nervous system demyelination secondary to infliximab therapy. A 47-year-old gentleman with a 15-year history of left sided ulcerative colitis presented to the gastroenterology clinic with a 1-month history of bloody diarrhoea associated with a significantly elevated faecal calprotectin. A trial of oral and rectal mesalazine as well as oral steroids proved ineffective. He had previously been intolerant to both Azathioprine and 6-mercaptopurine. Decision was made to escalate his treatment to methotrexate and infliximab 5 mg/kg (originator). He was managed in the outpatient setting and did not require hospitalization. First infliximab infusion was given on 14 May 2020. Second and third infusion were given two and six weeks after respectively. One week prior to the third infusion, he began to develop tingling and numbness down the right side of his body and he felt his right foot was more sensitive to changes in temperature. His Methotrexate was stopped but it was decided to proceed with giving the third infusion of infliximab. In the following two weeks he then developed weakness in the left leg and reported urinary hesitancy. He was reviewed in the ambulatory unit by the neurologist twelve days following the start of his neurological symptoms. On clinical examination, cranial nerves were intact. He had good muscle bulk and no focal wasting. Tone was normal bilaterally, but power was mildly reduced on the left, 4/5 in wrist, digits, hip flexion and knee extension. Reflexes were present bilaterally, but the supinator, knee and ankle reflexes were brisk on the left. Coordination was intact. There was reduced proprioception and temperature sensation on the right side, with a sensory level just below the clavicle, whilst touch, vibration and two-point discrimination were preserved bilaterally. Plantars were downgoing bilaterally. An urgent MRI of the spine was subsequently arranged which revealed a right sided intramedullary cord lesion at C4 with some focal eccentric enhancement (Figure 1). A subsequent MRI of his head revealed white matter plaques in the cerebral hemisphere and corpus callosum (Figure 2). The post contrast sequences (not shown) showed no features of active demyelination. CSF analysis was positive for IgG oligoclonal bands. Serum oligoclonal band testing revealed no abnormalities. These findings supported a diagnosis of Brown-Sequard syndrome secondary to a cord lesion due to multiple sclerosis (MS). The diagnosis of MS was based on evidence of widespread inflammation in the brain and the spinal cord in addition to positive oligoclonal bands in the CSF, which can be used as criteria for dissemination in time (2017 revised McDonald criteria). His infliximab was discontinued after his third infusion with no deterioration to his colitis and his neurology gradually started to improve two weeks later. He had a further flare of his MS a few months later manifesting as diplopia. Repeat MRI showed signal change involving the right deep parietal lobe that was more conspicuous than before probably representing some disease progression. Following discussion in the neuroinflammatory MDT it was decided that given the significant inflammatory activity he should be started on Natalizumab. Although this is not a licensed treatment for ulcerative colitis, being an anti-integrin, it was thought that it may also have the added benefit of reducing the risk of colitis flare. His first Natalizumab infusion was eight months after his last infliximab infusion.","PeriodicalId":17674,"journal":{"name":"JRSM Open","volume":"12 9","pages":"20542704211035987"},"PeriodicalIF":0.0000,"publicationDate":"2021-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/4a/10.1177_20542704211035987.PMC8411633.pdf","citationCount":"1","resultStr":"{\"title\":\"Hemi-paraplegia and hemi-anaesthesia in the inflammatory bowel disease clinic.\",\"authors\":\"Hesam Ahmadi Nooredinvand, Anu Vallipuram, Alice Dawson, Jaymin Patel, Waqar Rashid, Andrew Poullis\",\"doi\":\"10.1177/20542704211035987\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"In this case report, we present a rare case of central nervous system demyelination secondary to infliximab therapy. A 47-year-old gentleman with a 15-year history of left sided ulcerative colitis presented to the gastroenterology clinic with a 1-month history of bloody diarrhoea associated with a significantly elevated faecal calprotectin. A trial of oral and rectal mesalazine as well as oral steroids proved ineffective. He had previously been intolerant to both Azathioprine and 6-mercaptopurine. Decision was made to escalate his treatment to methotrexate and infliximab 5 mg/kg (originator). He was managed in the outpatient setting and did not require hospitalization. First infliximab infusion was given on 14 May 2020. Second and third infusion were given two and six weeks after respectively. One week prior to the third infusion, he began to develop tingling and numbness down the right side of his body and he felt his right foot was more sensitive to changes in temperature. His Methotrexate was stopped but it was decided to proceed with giving the third infusion of infliximab. In the following two weeks he then developed weakness in the left leg and reported urinary hesitancy. He was reviewed in the ambulatory unit by the neurologist twelve days following the start of his neurological symptoms. On clinical examination, cranial nerves were intact. He had good muscle bulk and no focal wasting. Tone was normal bilaterally, but power was mildly reduced on the left, 4/5 in wrist, digits, hip flexion and knee extension. Reflexes were present bilaterally, but the supinator, knee and ankle reflexes were brisk on the left. Coordination was intact. There was reduced proprioception and temperature sensation on the right side, with a sensory level just below the clavicle, whilst touch, vibration and two-point discrimination were preserved bilaterally. Plantars were downgoing bilaterally. An urgent MRI of the spine was subsequently arranged which revealed a right sided intramedullary cord lesion at C4 with some focal eccentric enhancement (Figure 1). A subsequent MRI of his head revealed white matter plaques in the cerebral hemisphere and corpus callosum (Figure 2). The post contrast sequences (not shown) showed no features of active demyelination. CSF analysis was positive for IgG oligoclonal bands. Serum oligoclonal band testing revealed no abnormalities. These findings supported a diagnosis of Brown-Sequard syndrome secondary to a cord lesion due to multiple sclerosis (MS). The diagnosis of MS was based on evidence of widespread inflammation in the brain and the spinal cord in addition to positive oligoclonal bands in the CSF, which can be used as criteria for dissemination in time (2017 revised McDonald criteria). His infliximab was discontinued after his third infusion with no deterioration to his colitis and his neurology gradually started to improve two weeks later. He had a further flare of his MS a few months later manifesting as diplopia. Repeat MRI showed signal change involving the right deep parietal lobe that was more conspicuous than before probably representing some disease progression. Following discussion in the neuroinflammatory MDT it was decided that given the significant inflammatory activity he should be started on Natalizumab. Although this is not a licensed treatment for ulcerative colitis, being an anti-integrin, it was thought that it may also have the added benefit of reducing the risk of colitis flare. His first Natalizumab infusion was eight months after his last infliximab infusion.\",\"PeriodicalId\":17674,\"journal\":{\"name\":\"JRSM Open\",\"volume\":\"12 9\",\"pages\":\"20542704211035987\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/4a/10.1177_20542704211035987.PMC8411633.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JRSM Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20542704211035987\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20542704211035987","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Hemi-paraplegia and hemi-anaesthesia in the inflammatory bowel disease clinic.
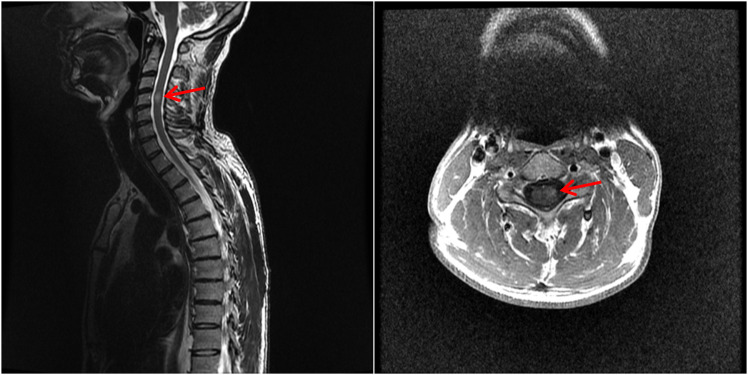
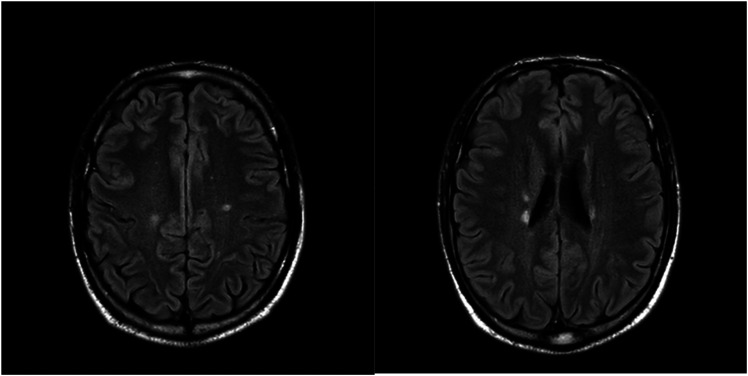
In this case report, we present a rare case of central nervous system demyelination secondary to infliximab therapy. A 47-year-old gentleman with a 15-year history of left sided ulcerative colitis presented to the gastroenterology clinic with a 1-month history of bloody diarrhoea associated with a significantly elevated faecal calprotectin. A trial of oral and rectal mesalazine as well as oral steroids proved ineffective. He had previously been intolerant to both Azathioprine and 6-mercaptopurine. Decision was made to escalate his treatment to methotrexate and infliximab 5 mg/kg (originator). He was managed in the outpatient setting and did not require hospitalization. First infliximab infusion was given on 14 May 2020. Second and third infusion were given two and six weeks after respectively. One week prior to the third infusion, he began to develop tingling and numbness down the right side of his body and he felt his right foot was more sensitive to changes in temperature. His Methotrexate was stopped but it was decided to proceed with giving the third infusion of infliximab. In the following two weeks he then developed weakness in the left leg and reported urinary hesitancy. He was reviewed in the ambulatory unit by the neurologist twelve days following the start of his neurological symptoms. On clinical examination, cranial nerves were intact. He had good muscle bulk and no focal wasting. Tone was normal bilaterally, but power was mildly reduced on the left, 4/5 in wrist, digits, hip flexion and knee extension. Reflexes were present bilaterally, but the supinator, knee and ankle reflexes were brisk on the left. Coordination was intact. There was reduced proprioception and temperature sensation on the right side, with a sensory level just below the clavicle, whilst touch, vibration and two-point discrimination were preserved bilaterally. Plantars were downgoing bilaterally. An urgent MRI of the spine was subsequently arranged which revealed a right sided intramedullary cord lesion at C4 with some focal eccentric enhancement (Figure 1). A subsequent MRI of his head revealed white matter plaques in the cerebral hemisphere and corpus callosum (Figure 2). The post contrast sequences (not shown) showed no features of active demyelination. CSF analysis was positive for IgG oligoclonal bands. Serum oligoclonal band testing revealed no abnormalities. These findings supported a diagnosis of Brown-Sequard syndrome secondary to a cord lesion due to multiple sclerosis (MS). The diagnosis of MS was based on evidence of widespread inflammation in the brain and the spinal cord in addition to positive oligoclonal bands in the CSF, which can be used as criteria for dissemination in time (2017 revised McDonald criteria). His infliximab was discontinued after his third infusion with no deterioration to his colitis and his neurology gradually started to improve two weeks later. He had a further flare of his MS a few months later manifesting as diplopia. Repeat MRI showed signal change involving the right deep parietal lobe that was more conspicuous than before probably representing some disease progression. Following discussion in the neuroinflammatory MDT it was decided that given the significant inflammatory activity he should be started on Natalizumab. Although this is not a licensed treatment for ulcerative colitis, being an anti-integrin, it was thought that it may also have the added benefit of reducing the risk of colitis flare. His first Natalizumab infusion was eight months after his last infliximab infusion.
期刊介绍:
JRSM Open is a peer reviewed online-only journal that follows the open-access publishing model. It is a companion journal to the Journal of the Royal Society of Medicine. The journal publishes research papers, research letters, clinical and methodological reviews, and case reports. Our aim is to inform practice and policy making in clinical medicine. The journal has an international and multispecialty readership that includes primary care and public health professionals.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
