Sebastian Zschätzsch, Manuela Stauss-Grabo, Adelheid Gauly, Jennifer Braun
{"title":"将容量状态监测和血容量控制超滤整合到体外肾替代治疗中。","authors":"Sebastian Zschätzsch, Manuela Stauss-Grabo, Adelheid Gauly, Jennifer Braun","doi":"10.2147/IJNRD.S319911","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Volume management in hemodialysis (HD) requires the ability to assess volume status objectively and determine treatment strategies that achieve euvolemia without compromising hemodynamic stability. The aim of this study was to compare dialysis with and without blood volume-controlled ultrafiltration (UF) in combination with body composition monitoring, and to evaluate indicators for adequate dialysis (Kt/V), ultrafiltration volume, fluid status, and the occurrence of intradialytic morbid events (IME).</p><p><strong>Patients and methods: </strong>Patients undergoing hemodialysis or on-line hemodiafiltration with support of a blood volume monitor (BVM) - a feedback control device integrated into the 5008 and 6008 HD systems - were enrolled. Patients received treatment for four weeks using the 6008 CAREsystem and the BVM (6008+). Data on dialysis dose (Kt/V), UF volume and predialysis fluid status were documented. This data was also documented retrospectively for four weeks with (5008+) and without (5008-) the use of the BVM with the 5008 system. Comparisons were analyzed using linear mixed models.</p><p><strong>Results: </strong>Twenty-four patients were enrolled. Kt/V was unaffected by blood volume-controlled UF (5008- vs 5008+: <i>p</i>=0.230) and was equally achieved with both HD systems (5008+ vs 6008+: <i>p</i>=0.922). The UF volume and fluid status achieved were comparable, independent of the use of UF control with BVM (5008- vs 5008+; UF volume: <i>p</i>=0.166; fluid overload: <i>p</i>=0.390) or the HD system (5008+ vs 6008+: UF volume: <i>p</i>=0.003; fluid overload: <i>p</i>=0.838), except for UF volume being higher in the 6008+ phase. IMEs occurred in less than 3% of treatments, with no difference between study phases.</p><p><strong>Conclusion: </strong>This study demonstrates that a clinical approach to kidney replacement therapy that tracks volume status and manages intradialytic fluid removal by blood volume-controlled UF delivers adequate dialysis without compromising fluid removal. It maintains volume status and ensures low incidence of IMEs.</p>","PeriodicalId":14181,"journal":{"name":"International Journal of Nephrology and Renovascular Disease","volume":"14 ","pages":"349-358"},"PeriodicalIF":2.5000,"publicationDate":"2021-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/34/b2/ijnrd-14-349.PMC8416185.pdf","citationCount":"1","resultStr":"{\"title\":\"Integrating Monitoring of Volume Status and Blood Volume-Controlled Ultrafiltration into Extracorporeal Kidney Replacement Therapy.\",\"authors\":\"Sebastian Zschätzsch, Manuela Stauss-Grabo, Adelheid Gauly, Jennifer Braun\",\"doi\":\"10.2147/IJNRD.S319911\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Volume management in hemodialysis (HD) requires the ability to assess volume status objectively and determine treatment strategies that achieve euvolemia without compromising hemodynamic stability. The aim of this study was to compare dialysis with and without blood volume-controlled ultrafiltration (UF) in combination with body composition monitoring, and to evaluate indicators for adequate dialysis (Kt/V), ultrafiltration volume, fluid status, and the occurrence of intradialytic morbid events (IME).</p><p><strong>Patients and methods: </strong>Patients undergoing hemodialysis or on-line hemodiafiltration with support of a blood volume monitor (BVM) - a feedback control device integrated into the 5008 and 6008 HD systems - were enrolled. Patients received treatment for four weeks using the 6008 CAREsystem and the BVM (6008+). Data on dialysis dose (Kt/V), UF volume and predialysis fluid status were documented. This data was also documented retrospectively for four weeks with (5008+) and without (5008-) the use of the BVM with the 5008 system. Comparisons were analyzed using linear mixed models.</p><p><strong>Results: </strong>Twenty-four patients were enrolled. Kt/V was unaffected by blood volume-controlled UF (5008- vs 5008+: <i>p</i>=0.230) and was equally achieved with both HD systems (5008+ vs 6008+: <i>p</i>=0.922). The UF volume and fluid status achieved were comparable, independent of the use of UF control with BVM (5008- vs 5008+; UF volume: <i>p</i>=0.166; fluid overload: <i>p</i>=0.390) or the HD system (5008+ vs 6008+: UF volume: <i>p</i>=0.003; fluid overload: <i>p</i>=0.838), except for UF volume being higher in the 6008+ phase. IMEs occurred in less than 3% of treatments, with no difference between study phases.</p><p><strong>Conclusion: </strong>This study demonstrates that a clinical approach to kidney replacement therapy that tracks volume status and manages intradialytic fluid removal by blood volume-controlled UF delivers adequate dialysis without compromising fluid removal. It maintains volume status and ensures low incidence of IMEs.</p>\",\"PeriodicalId\":14181,\"journal\":{\"name\":\"International Journal of Nephrology and Renovascular Disease\",\"volume\":\"14 \",\"pages\":\"349-358\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2021-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/34/b2/ijnrd-14-349.PMC8416185.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Nephrology and Renovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/IJNRD.S319911\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Nephrology and Renovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/IJNRD.S319911","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 1
摘要
目的:血液透析(HD)的容量管理需要客观评估容量状态的能力,并确定在不影响血流动力学稳定性的情况下实现euvolemia的治疗策略。本研究的目的是比较使用和不使用血容量控制超滤(UF)结合体成分监测的透析,并评估充分透析(Kt/V)、超滤体积、液体状态和透析内发病事件(IME)发生的指标。患者和方法:患者接受血液透析或在线血液滤过,支持血容量监测仪(BVM) -一个集成到5008和6008 HD系统的反馈控制装置-入组。患者使用6008 CAREsystem和BVM(6008+)进行为期四周的治疗。记录透析剂量(Kt/V)、UF体积和透析前液体状态的数据。回顾性记录了在(5008+)和(5008-)情况下使用BVM和5008系统的四周数据。采用线性混合模型进行比较分析。结果:24例患者入组。Kt/V不受血容量控制UF的影响(5008- vs 5008+: p=0.230),两种HD系统均可达到相同的效果(5008+ vs 6008+: p=0.922)。所获得的UF体积和流体状态具有可比性,独立于使用UF控制与BVM (5008- vs 5008+;UF体积:p=0.166;流体过载:p=0.390)或HD系统(5008+ vs 6008+: UF体积:p=0.003;流体过载:p=0.838),除了6008+阶段UF体积更高。在不到3%的治疗中发生了ime,研究阶段之间没有差异。结论:本研究表明,一种临床方法的肾脏替代疗法,跟踪容量状态和管理透析内液体清除通过血容量控制UF提供充分的透析而不影响液体清除。它保持体积状态,并确保低发生率的ime。
Integrating Monitoring of Volume Status and Blood Volume-Controlled Ultrafiltration into Extracorporeal Kidney Replacement Therapy.
Purpose: Volume management in hemodialysis (HD) requires the ability to assess volume status objectively and determine treatment strategies that achieve euvolemia without compromising hemodynamic stability. The aim of this study was to compare dialysis with and without blood volume-controlled ultrafiltration (UF) in combination with body composition monitoring, and to evaluate indicators for adequate dialysis (Kt/V), ultrafiltration volume, fluid status, and the occurrence of intradialytic morbid events (IME).
Patients and methods: Patients undergoing hemodialysis or on-line hemodiafiltration with support of a blood volume monitor (BVM) - a feedback control device integrated into the 5008 and 6008 HD systems - were enrolled. Patients received treatment for four weeks using the 6008 CAREsystem and the BVM (6008+). Data on dialysis dose (Kt/V), UF volume and predialysis fluid status were documented. This data was also documented retrospectively for four weeks with (5008+) and without (5008-) the use of the BVM with the 5008 system. Comparisons were analyzed using linear mixed models.
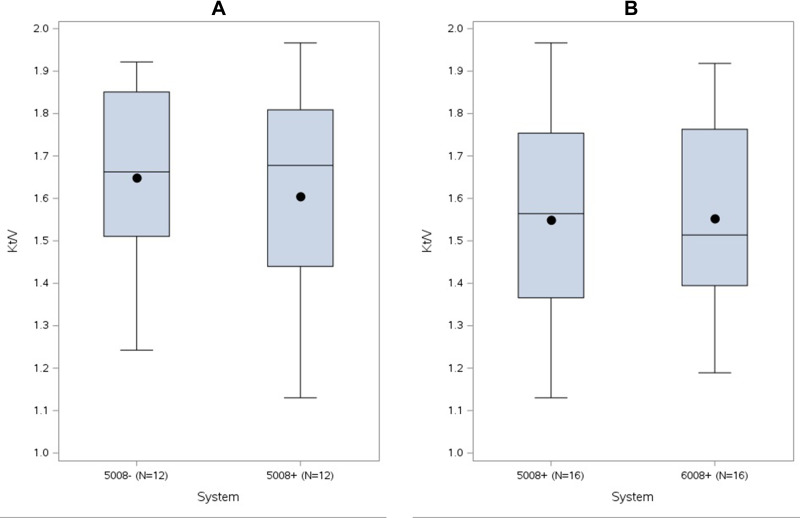
Results: Twenty-four patients were enrolled. Kt/V was unaffected by blood volume-controlled UF (5008- vs 5008+: p=0.230) and was equally achieved with both HD systems (5008+ vs 6008+: p=0.922). The UF volume and fluid status achieved were comparable, independent of the use of UF control with BVM (5008- vs 5008+; UF volume: p=0.166; fluid overload: p=0.390) or the HD system (5008+ vs 6008+: UF volume: p=0.003; fluid overload: p=0.838), except for UF volume being higher in the 6008+ phase. IMEs occurred in less than 3% of treatments, with no difference between study phases.
Conclusion: This study demonstrates that a clinical approach to kidney replacement therapy that tracks volume status and manages intradialytic fluid removal by blood volume-controlled UF delivers adequate dialysis without compromising fluid removal. It maintains volume status and ensures low incidence of IMEs.
期刊介绍:
International Journal of Nephrology and Renovascular Disease is an international, peer-reviewed, open-access journal focusing on the pathophysiology of the kidney and vascular supply. Epidemiology, screening, diagnosis, and treatment interventions are covered as well as basic science, biochemical and immunological studies. In particular, emphasis will be given to: -Chronic kidney disease- Complications of renovascular disease- Imaging techniques- Renal hypertension- Renal cancer- Treatment including pharmacological and transplantation- Dialysis and treatment of complications of dialysis and renal disease- Quality of Life- Patient satisfaction and preference- Health economic evaluations. The journal welcomes submitted papers covering original research, basic science, clinical studies, reviews & evaluations, guidelines, expert opinion and commentary, case reports and extended reports. The main focus of the journal will be to publish research and clinical results in humans but preclinical, animal and in vitro studies will be published where they shed light on disease processes and potential new therapies and interventions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
