Joseph Newton, Lauren Floyd, Arvind Ponnusamy, John Anderton
{"title":"继发于复发性前列腺癌的血栓性微血管病。","authors":"Joseph Newton, Lauren Floyd, Arvind Ponnusamy, John Anderton","doi":"10.5414/CNCS110609","DOIUrl":null,"url":null,"abstract":"<p><p>An 86-year-old man returned to the UK from Spain with symptoms suggestive of gastrointestinal bleeding. He was found to have an acute kidney injury and thrombocytopenia. Further investigations identified the presence of a microangiopathic hemolytic anemia, supporting the diagnosis of a thrombotic microangiopathy. Differentials included atypical hemolytic uremic syndrome and secondary thrombotic microangiopathy. Thrombotic thrombocytopenic purpura (TTP) and STEC (Shiga toxin-producing <i>E. coli</i>) hemolytic uremic syndrome were excluded by a normal ADAMTS-13 and negative <i>E. coli</i> serology and stool PCR. The patient was treated with blood and platelet transfusions. He received eculizumab and hemodialysis whilst a screen for secondary causes was undertaken. Thrombotic microangiopathy was shown to be secondary to recurrence of prostate cancer, which had been treated 16 years previously. He later recovered his renal function and receives ongoing hormonal treatment for his prostate cancer.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"9 ","pages":"105-109"},"PeriodicalIF":0.0000,"publicationDate":"2021-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8443975/pdf/","citationCount":"0","resultStr":"{\"title\":\"Thrombotic microangiopathy secondary to recurrent prostate cancer.\",\"authors\":\"Joseph Newton, Lauren Floyd, Arvind Ponnusamy, John Anderton\",\"doi\":\"10.5414/CNCS110609\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>An 86-year-old man returned to the UK from Spain with symptoms suggestive of gastrointestinal bleeding. He was found to have an acute kidney injury and thrombocytopenia. Further investigations identified the presence of a microangiopathic hemolytic anemia, supporting the diagnosis of a thrombotic microangiopathy. Differentials included atypical hemolytic uremic syndrome and secondary thrombotic microangiopathy. Thrombotic thrombocytopenic purpura (TTP) and STEC (Shiga toxin-producing <i>E. coli</i>) hemolytic uremic syndrome were excluded by a normal ADAMTS-13 and negative <i>E. coli</i> serology and stool PCR. The patient was treated with blood and platelet transfusions. He received eculizumab and hemodialysis whilst a screen for secondary causes was undertaken. Thrombotic microangiopathy was shown to be secondary to recurrence of prostate cancer, which had been treated 16 years previously. He later recovered his renal function and receives ongoing hormonal treatment for his prostate cancer.</p>\",\"PeriodicalId\":10398,\"journal\":{\"name\":\"Clinical Nephrology. Case Studies\",\"volume\":\"9 \",\"pages\":\"105-109\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-09-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8443975/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Nephrology. Case Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS110609\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110609","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Thrombotic microangiopathy secondary to recurrent prostate cancer.
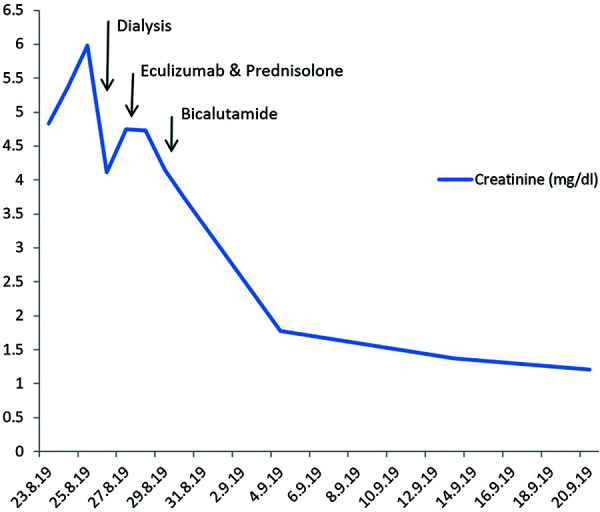
An 86-year-old man returned to the UK from Spain with symptoms suggestive of gastrointestinal bleeding. He was found to have an acute kidney injury and thrombocytopenia. Further investigations identified the presence of a microangiopathic hemolytic anemia, supporting the diagnosis of a thrombotic microangiopathy. Differentials included atypical hemolytic uremic syndrome and secondary thrombotic microangiopathy. Thrombotic thrombocytopenic purpura (TTP) and STEC (Shiga toxin-producing E. coli) hemolytic uremic syndrome were excluded by a normal ADAMTS-13 and negative E. coli serology and stool PCR. The patient was treated with blood and platelet transfusions. He received eculizumab and hemodialysis whilst a screen for secondary causes was undertaken. Thrombotic microangiopathy was shown to be secondary to recurrence of prostate cancer, which had been treated 16 years previously. He later recovered his renal function and receives ongoing hormonal treatment for his prostate cancer.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
