Shufeng Tian, Jikui Deng, Wenhua Huang, Linlin Liu, Yunsheng Chen, Yongqiang Jiang, Gang Liu
{"title":"FAM89A 和 IFI44L 用于区分发热患儿的病毒感染和细菌感染。","authors":"Shufeng Tian, Jikui Deng, Wenhua Huang, Linlin Liu, Yunsheng Chen, Yongqiang Jiang, Gang Liu","doi":"10.1002/ped4.12295","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>The current lack of reliable rapid tests for distinguishing between bacterial and viral infections has contributed to antibiotic misuse.</p><p><strong>Objective: </strong>This study aimed to develop a novel biomarker assay that integrates <i>FAM89A</i> and <i>IFI44L</i> measurements to assist in differentiating between bacterial and viral infections.</p><p><strong>Methods: </strong>This prospective study recruited children with febrile illness from two hospitals between July 1, 2018, and June 30, 2019. A panel of three experienced pediatricians performed reference standard diagnoses of all patients (i.e., bacterial or viral infection) using available clinical and laboratory data, including a 28-day follow-up assessment. Assay operators were blinded to the reference standard diagnoses. The expression levels of <i>FAM89A</i> and <i>IFI44L</i> were determined by quantitative real-time polymerase chain reaction assessment.</p><p><strong>Results: </strong>Of 133 potentially eligible patients with suspected bacterial or viral infection, 35 were excluded after the application of exclusion criteria. The resulting cohort included 98 patients: 59 with viral diagnoses and 39 with bacterial diagnoses. The areas under the curve (AUCs) of diagnoses using <i>FAM89A</i> and <i>IFI44L</i> were 0.694 [95% confidence interval (<i>CI</i>): 0.583-0.804] and 0.751 (95% <i>CI</i>: 0.651-0.851), respectively. The disease risk score (DRS) [log<sub>2</sub>(<i>FAM89A</i> expression) - log<sub>2</sub>(<i>IFI44L</i> expression)] signature achieved an improved area under the receiver operating characteristic curve (AUC, 0.825; 95% <i>CI</i>: 0.735-0.915), compared with the AUC generated from individual host RNA. A combination of the DRS and the C-reactive protein (CRP) level achieved an AUC of 0.896 (95% <i>CI</i>: 0.825-0.966). Optimal cutoffs for the DRS and CRP level were -3.18 and 19.80 mg/L, respectively.</p><p><strong>Interpretation: </strong>The DRS was significantly more accurate than the CRP level in distinguishing between bacterial and viral infections; the combination of these two parameters exhibited greater sensitivity and specificity. This study provides information that could be useful for the clinical application of <i>FAM89A</i> and <i>IFI44L</i> in terms of distinguishing between viral and bacterial infections.</p>","PeriodicalId":19992,"journal":{"name":"Pediatric Investigation","volume":"5 3","pages":"195-202"},"PeriodicalIF":2.0000,"publicationDate":"2021-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/37/01/PED4-5-195.PMC8458721.pdf","citationCount":"0","resultStr":"{\"title\":\"<i>FAM89A</i> and <i>IFI44L</i> for distinguishing between viral and bacterial infections in children with febrile illness.\",\"authors\":\"Shufeng Tian, Jikui Deng, Wenhua Huang, Linlin Liu, Yunsheng Chen, Yongqiang Jiang, Gang Liu\",\"doi\":\"10.1002/ped4.12295\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>The current lack of reliable rapid tests for distinguishing between bacterial and viral infections has contributed to antibiotic misuse.</p><p><strong>Objective: </strong>This study aimed to develop a novel biomarker assay that integrates <i>FAM89A</i> and <i>IFI44L</i> measurements to assist in differentiating between bacterial and viral infections.</p><p><strong>Methods: </strong>This prospective study recruited children with febrile illness from two hospitals between July 1, 2018, and June 30, 2019. A panel of three experienced pediatricians performed reference standard diagnoses of all patients (i.e., bacterial or viral infection) using available clinical and laboratory data, including a 28-day follow-up assessment. Assay operators were blinded to the reference standard diagnoses. The expression levels of <i>FAM89A</i> and <i>IFI44L</i> were determined by quantitative real-time polymerase chain reaction assessment.</p><p><strong>Results: </strong>Of 133 potentially eligible patients with suspected bacterial or viral infection, 35 were excluded after the application of exclusion criteria. The resulting cohort included 98 patients: 59 with viral diagnoses and 39 with bacterial diagnoses. The areas under the curve (AUCs) of diagnoses using <i>FAM89A</i> and <i>IFI44L</i> were 0.694 [95% confidence interval (<i>CI</i>): 0.583-0.804] and 0.751 (95% <i>CI</i>: 0.651-0.851), respectively. The disease risk score (DRS) [log<sub>2</sub>(<i>FAM89A</i> expression) - log<sub>2</sub>(<i>IFI44L</i> expression)] signature achieved an improved area under the receiver operating characteristic curve (AUC, 0.825; 95% <i>CI</i>: 0.735-0.915), compared with the AUC generated from individual host RNA. A combination of the DRS and the C-reactive protein (CRP) level achieved an AUC of 0.896 (95% <i>CI</i>: 0.825-0.966). Optimal cutoffs for the DRS and CRP level were -3.18 and 19.80 mg/L, respectively.</p><p><strong>Interpretation: </strong>The DRS was significantly more accurate than the CRP level in distinguishing between bacterial and viral infections; the combination of these two parameters exhibited greater sensitivity and specificity. This study provides information that could be useful for the clinical application of <i>FAM89A</i> and <i>IFI44L</i> in terms of distinguishing between viral and bacterial infections.</p>\",\"PeriodicalId\":19992,\"journal\":{\"name\":\"Pediatric Investigation\",\"volume\":\"5 3\",\"pages\":\"195-202\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2021-09-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/37/01/PED4-5-195.PMC8458721.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Investigation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/ped4.12295\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Investigation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ped4.12295","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
FAM89A and IFI44L for distinguishing between viral and bacterial infections in children with febrile illness.
Importance: The current lack of reliable rapid tests for distinguishing between bacterial and viral infections has contributed to antibiotic misuse.
Objective: This study aimed to develop a novel biomarker assay that integrates FAM89A and IFI44L measurements to assist in differentiating between bacterial and viral infections.
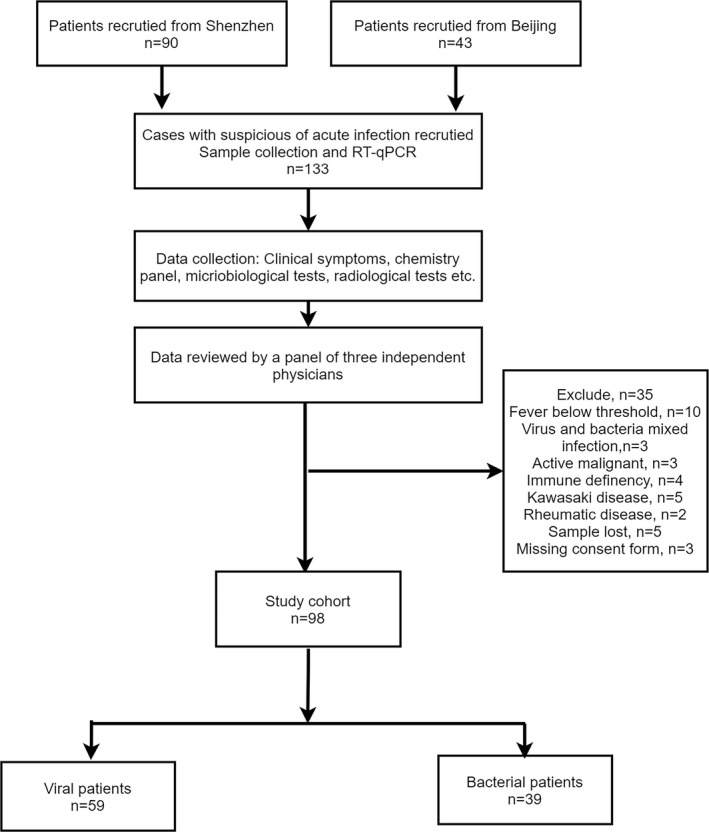
Methods: This prospective study recruited children with febrile illness from two hospitals between July 1, 2018, and June 30, 2019. A panel of three experienced pediatricians performed reference standard diagnoses of all patients (i.e., bacterial or viral infection) using available clinical and laboratory data, including a 28-day follow-up assessment. Assay operators were blinded to the reference standard diagnoses. The expression levels of FAM89A and IFI44L were determined by quantitative real-time polymerase chain reaction assessment.
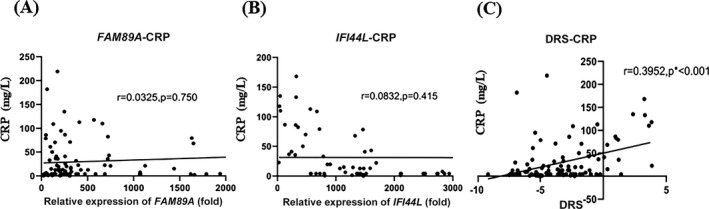
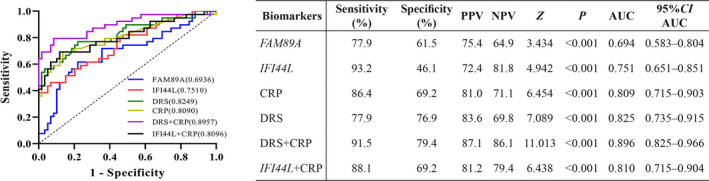
Results: Of 133 potentially eligible patients with suspected bacterial or viral infection, 35 were excluded after the application of exclusion criteria. The resulting cohort included 98 patients: 59 with viral diagnoses and 39 with bacterial diagnoses. The areas under the curve (AUCs) of diagnoses using FAM89A and IFI44L were 0.694 [95% confidence interval (CI): 0.583-0.804] and 0.751 (95% CI: 0.651-0.851), respectively. The disease risk score (DRS) [log2(FAM89A expression) - log2(IFI44L expression)] signature achieved an improved area under the receiver operating characteristic curve (AUC, 0.825; 95% CI: 0.735-0.915), compared with the AUC generated from individual host RNA. A combination of the DRS and the C-reactive protein (CRP) level achieved an AUC of 0.896 (95% CI: 0.825-0.966). Optimal cutoffs for the DRS and CRP level were -3.18 and 19.80 mg/L, respectively.
Interpretation: The DRS was significantly more accurate than the CRP level in distinguishing between bacterial and viral infections; the combination of these two parameters exhibited greater sensitivity and specificity. This study provides information that could be useful for the clinical application of FAM89A and IFI44L in terms of distinguishing between viral and bacterial infections.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
