Jong Han Gill, Taek Kyun Nam, Hoon Kyo Jung, Kyung Min Jang, Hyun Ho Choi, Yong Sook Park, Jeong Taik Kwon
{"title":"烟雾综合征和格雷夫斯病患者急性脑梗死合并甲状腺风暴。","authors":"Jong Han Gill, Taek Kyun Nam, Hoon Kyo Jung, Kyung Min Jang, Hyun Ho Choi, Yong Sook Park, Jeong Taik Kwon","doi":"10.7461/jcen.2021.E2021.07.003","DOIUrl":null,"url":null,"abstract":"<p><p>Moyamoya syndrome (MMS) associated with hyperthyroidism, such as Graves' disease, is a rare condition that causes ischemic stroke with thyrotoxicity. A 43-year-old woman with symptoms of right hemiparesis was admitted. Brain magnetic resonance imaging revealed a small cerebral infarction in the left frontal lobe. Cerebral angiography revealed multi-vessel intracranial occlusive disease. Several days later, neurologic deterioration and aggravation of cerebral infarction developed due to a thyroid storm. A thyroid function test revealed the following: thyroid-stimulating hormone (TSH) <0.01 μunits/mL (reference range, 0.55-4.78 μunits/mL); triiodo-thyronine >8.0 ng/mL (reference range, 0.77-1.81 ng/mL); free thyroxine (T4) of 9.47 pmol/L (reference range, 11.4-22.6 pmol/L); and TSH receptor antibody of 37.10 U/L (reference range, 0-10 U/L). For thyroid storm management, we initiated treatment with methimazole, Gemstein's solution, and hydrocortisone. Finally, the thyroid disease was controlled, and neurologic deficits improved. We describe a case of acute cerebral infarction combined with a thyroid storm in a patient with Moyamoya syndrome and Graves' disease. Hyperthyroidism such as Graves' disease should be considered in the differential diagnosis for patho-etiologic mechanisms associated with MMS. A cerebrovascular disease with a thyroid storm can lead to severe mortality and morbidity. Prompt diagnosis and strict treatment are important.</p>","PeriodicalId":15359,"journal":{"name":"Journal of Cerebrovascular and Endovascular Neurosurgery","volume":" ","pages":"160-165"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/2b/jcen-2021-e2021-07-003.PMC9260458.pdf","citationCount":"3","resultStr":"{\"title\":\"Acute cerebral infarction combined with a thyroid storm in a patient with both Moyamoya syndrome and Graves' disease.\",\"authors\":\"Jong Han Gill, Taek Kyun Nam, Hoon Kyo Jung, Kyung Min Jang, Hyun Ho Choi, Yong Sook Park, Jeong Taik Kwon\",\"doi\":\"10.7461/jcen.2021.E2021.07.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Moyamoya syndrome (MMS) associated with hyperthyroidism, such as Graves' disease, is a rare condition that causes ischemic stroke with thyrotoxicity. A 43-year-old woman with symptoms of right hemiparesis was admitted. Brain magnetic resonance imaging revealed a small cerebral infarction in the left frontal lobe. Cerebral angiography revealed multi-vessel intracranial occlusive disease. Several days later, neurologic deterioration and aggravation of cerebral infarction developed due to a thyroid storm. A thyroid function test revealed the following: thyroid-stimulating hormone (TSH) <0.01 μunits/mL (reference range, 0.55-4.78 μunits/mL); triiodo-thyronine >8.0 ng/mL (reference range, 0.77-1.81 ng/mL); free thyroxine (T4) of 9.47 pmol/L (reference range, 11.4-22.6 pmol/L); and TSH receptor antibody of 37.10 U/L (reference range, 0-10 U/L). For thyroid storm management, we initiated treatment with methimazole, Gemstein's solution, and hydrocortisone. Finally, the thyroid disease was controlled, and neurologic deficits improved. We describe a case of acute cerebral infarction combined with a thyroid storm in a patient with Moyamoya syndrome and Graves' disease. Hyperthyroidism such as Graves' disease should be considered in the differential diagnosis for patho-etiologic mechanisms associated with MMS. A cerebrovascular disease with a thyroid storm can lead to severe mortality and morbidity. Prompt diagnosis and strict treatment are important.</p>\",\"PeriodicalId\":15359,\"journal\":{\"name\":\"Journal of Cerebrovascular and Endovascular Neurosurgery\",\"volume\":\" \",\"pages\":\"160-165\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/2b/jcen-2021-e2021-07-003.PMC9260458.pdf\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cerebrovascular and Endovascular Neurosurgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7461/jcen.2021.E2021.07.003\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/10/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cerebrovascular and Endovascular Neurosurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7461/jcen.2021.E2021.07.003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/10/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Acute cerebral infarction combined with a thyroid storm in a patient with both Moyamoya syndrome and Graves' disease.
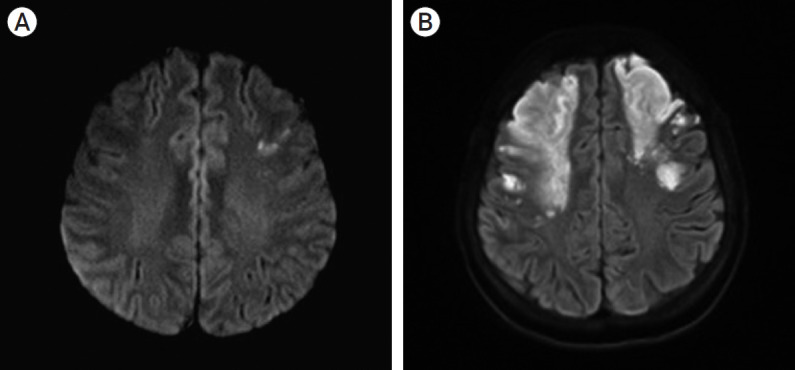
Moyamoya syndrome (MMS) associated with hyperthyroidism, such as Graves' disease, is a rare condition that causes ischemic stroke with thyrotoxicity. A 43-year-old woman with symptoms of right hemiparesis was admitted. Brain magnetic resonance imaging revealed a small cerebral infarction in the left frontal lobe. Cerebral angiography revealed multi-vessel intracranial occlusive disease. Several days later, neurologic deterioration and aggravation of cerebral infarction developed due to a thyroid storm. A thyroid function test revealed the following: thyroid-stimulating hormone (TSH) <0.01 μunits/mL (reference range, 0.55-4.78 μunits/mL); triiodo-thyronine >8.0 ng/mL (reference range, 0.77-1.81 ng/mL); free thyroxine (T4) of 9.47 pmol/L (reference range, 11.4-22.6 pmol/L); and TSH receptor antibody of 37.10 U/L (reference range, 0-10 U/L). For thyroid storm management, we initiated treatment with methimazole, Gemstein's solution, and hydrocortisone. Finally, the thyroid disease was controlled, and neurologic deficits improved. We describe a case of acute cerebral infarction combined with a thyroid storm in a patient with Moyamoya syndrome and Graves' disease. Hyperthyroidism such as Graves' disease should be considered in the differential diagnosis for patho-etiologic mechanisms associated with MMS. A cerebrovascular disease with a thyroid storm can lead to severe mortality and morbidity. Prompt diagnosis and strict treatment are important.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
