Amina El Saghir, Georgios Dimitriou, Miriam Scholer, Ioanna Istampoulouoglou, Patrick Heinrich, Klaus Baumgartl, René Schwendimann, Stefano Bassetti, Anne Leuppi-Taegtmeyer
{"title":"在瑞士一家大学医院开发并实施药物不良事件电子触发工具。","authors":"Amina El Saghir, Georgios Dimitriou, Miriam Scholer, Ioanna Istampoulouoglou, Patrick Heinrich, Klaus Baumgartl, René Schwendimann, Stefano Bassetti, Anne Leuppi-Taegtmeyer","doi":"10.2147/DHPS.S334987","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The purpose of the study was to develop and implement an institution-specific trigger tool based on the Institute for Healthcare Improvement medication module trigger tool (IHI MMTT) in order to detect and monitor ADEs.</p><p><strong>Methods: </strong>We performed an investigator-driven, single-center study using retrospective and prospective patient data to develop (\"development phase\") and implement (\"implementation phase\") an efficient, institution-specific trigger tool based on the IHI MMTT. Complete medical data from 1008 patients hospitalized in 2018 were used in the development phase. ADEs were identified by chart review. The performance of two versions of the tool was assessed by comparing their sensitivities and specificities. Tool A employed only digitally extracted triggers (\"e-trigger-tool\") while Tool B employed an additional manually extracted trigger. The superior tool - taking efficiency into account - was applied prospectively to 19-22 randomly chosen charts per month for 26 months during the implementation phase.</p><p><strong>Results: </strong>In the development phase, 189 (19%) patients had ≥1 ADE (total 277 ADEs). The time needed to identify these ADEs was 15 minutes/chart. A total of 203 patients had ≥1 trigger (total 273 triggers - Tool B). The sensitivities and specificities of Tools A and B were 0.41 and 0.86, and 0.43 and 0.86, respectively. Tool A was more time-efficient than Tool B (4 vs 9 minutes/chart) and was therefore used in the implementation phase. During the 26-month implementation phase, 22 patients experienced trigger-identified ADEs and 529 did not. The median number of ADEs per 1000 patient days was 6 (range 0-13). Patients with at least one ADE had a mean hospital stay of 22.3 ± 19.7 days, compared to 8.0 ± 7.6 days for those without an ADE (p = 2.7×10<sup>-14</sup>).</p><p><strong>Conclusion: </strong>We developed and implemented an e-trigger tool that was specific and moderately sensitive, gave consistent results and required minimal resources.</p>","PeriodicalId":11377,"journal":{"name":"Drug, Healthcare and Patient Safety","volume":"13 ","pages":"251-263"},"PeriodicalIF":3.4000,"publicationDate":"2021-12-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5a/ca/dhps-13-251.PMC8713708.pdf","citationCount":"0","resultStr":"{\"title\":\"Development and Implementation of an e-Trigger Tool for Adverse Drug Events in a Swiss University Hospital.\",\"authors\":\"Amina El Saghir, Georgios Dimitriou, Miriam Scholer, Ioanna Istampoulouoglou, Patrick Heinrich, Klaus Baumgartl, René Schwendimann, Stefano Bassetti, Anne Leuppi-Taegtmeyer\",\"doi\":\"10.2147/DHPS.S334987\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The purpose of the study was to develop and implement an institution-specific trigger tool based on the Institute for Healthcare Improvement medication module trigger tool (IHI MMTT) in order to detect and monitor ADEs.</p><p><strong>Methods: </strong>We performed an investigator-driven, single-center study using retrospective and prospective patient data to develop (\\\"development phase\\\") and implement (\\\"implementation phase\\\") an efficient, institution-specific trigger tool based on the IHI MMTT. Complete medical data from 1008 patients hospitalized in 2018 were used in the development phase. ADEs were identified by chart review. The performance of two versions of the tool was assessed by comparing their sensitivities and specificities. Tool A employed only digitally extracted triggers (\\\"e-trigger-tool\\\") while Tool B employed an additional manually extracted trigger. The superior tool - taking efficiency into account - was applied prospectively to 19-22 randomly chosen charts per month for 26 months during the implementation phase.</p><p><strong>Results: </strong>In the development phase, 189 (19%) patients had ≥1 ADE (total 277 ADEs). The time needed to identify these ADEs was 15 minutes/chart. A total of 203 patients had ≥1 trigger (total 273 triggers - Tool B). The sensitivities and specificities of Tools A and B were 0.41 and 0.86, and 0.43 and 0.86, respectively. Tool A was more time-efficient than Tool B (4 vs 9 minutes/chart) and was therefore used in the implementation phase. During the 26-month implementation phase, 22 patients experienced trigger-identified ADEs and 529 did not. The median number of ADEs per 1000 patient days was 6 (range 0-13). Patients with at least one ADE had a mean hospital stay of 22.3 ± 19.7 days, compared to 8.0 ± 7.6 days for those without an ADE (p = 2.7×10<sup>-14</sup>).</p><p><strong>Conclusion: </strong>We developed and implemented an e-trigger tool that was specific and moderately sensitive, gave consistent results and required minimal resources.</p>\",\"PeriodicalId\":11377,\"journal\":{\"name\":\"Drug, Healthcare and Patient Safety\",\"volume\":\"13 \",\"pages\":\"251-263\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2021-12-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5a/ca/dhps-13-251.PMC8713708.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drug, Healthcare and Patient Safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/DHPS.S334987\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug, Healthcare and Patient Safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/DHPS.S334987","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Development and Implementation of an e-Trigger Tool for Adverse Drug Events in a Swiss University Hospital.
Purpose: The purpose of the study was to develop and implement an institution-specific trigger tool based on the Institute for Healthcare Improvement medication module trigger tool (IHI MMTT) in order to detect and monitor ADEs.
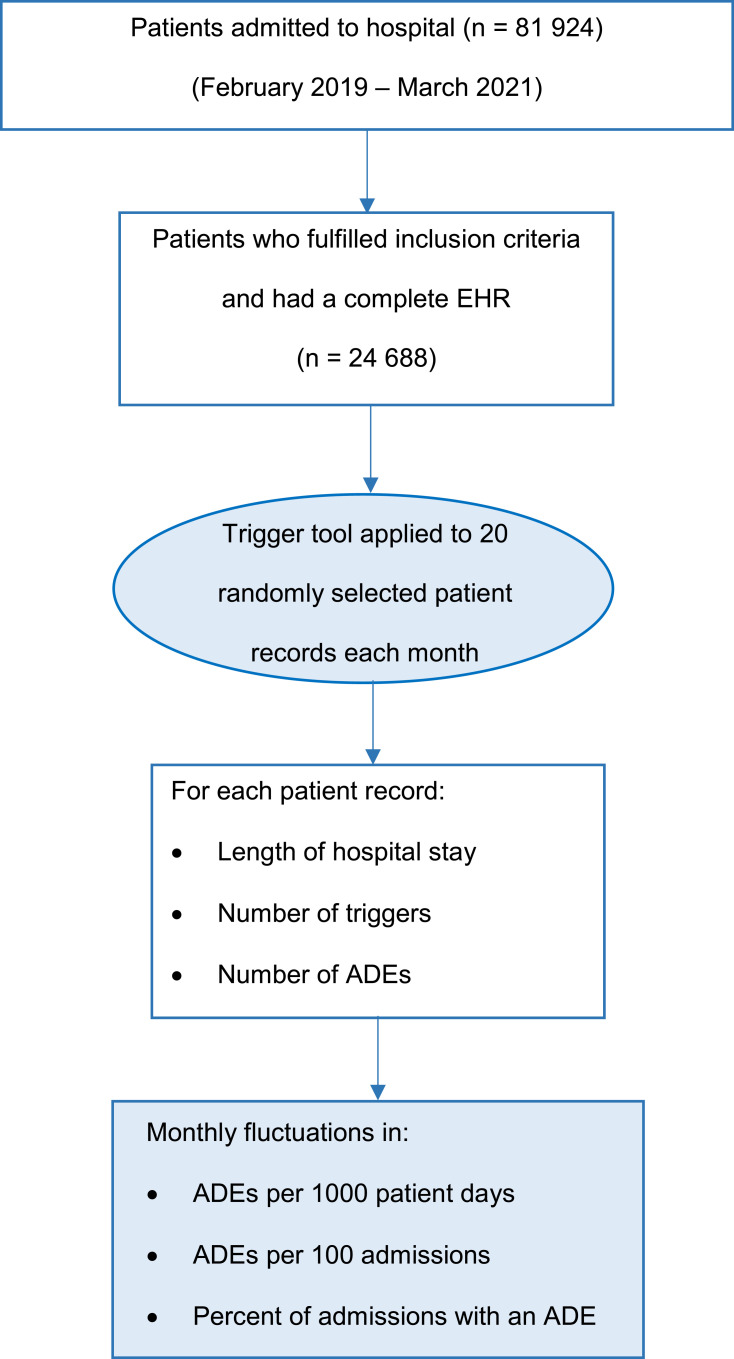
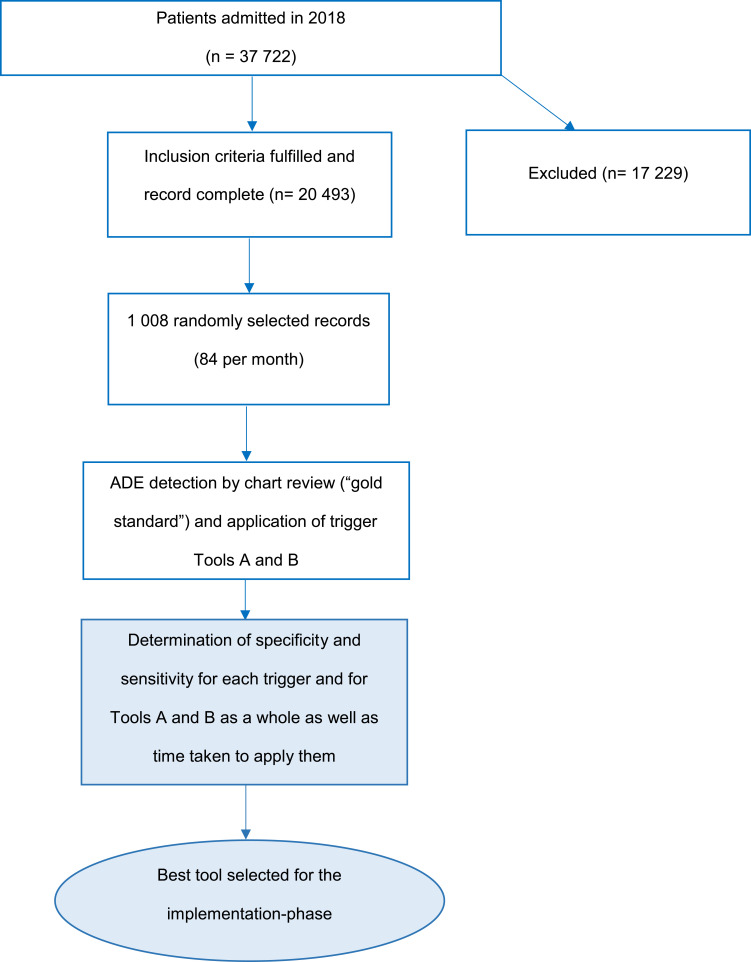
Methods: We performed an investigator-driven, single-center study using retrospective and prospective patient data to develop ("development phase") and implement ("implementation phase") an efficient, institution-specific trigger tool based on the IHI MMTT. Complete medical data from 1008 patients hospitalized in 2018 were used in the development phase. ADEs were identified by chart review. The performance of two versions of the tool was assessed by comparing their sensitivities and specificities. Tool A employed only digitally extracted triggers ("e-trigger-tool") while Tool B employed an additional manually extracted trigger. The superior tool - taking efficiency into account - was applied prospectively to 19-22 randomly chosen charts per month for 26 months during the implementation phase.
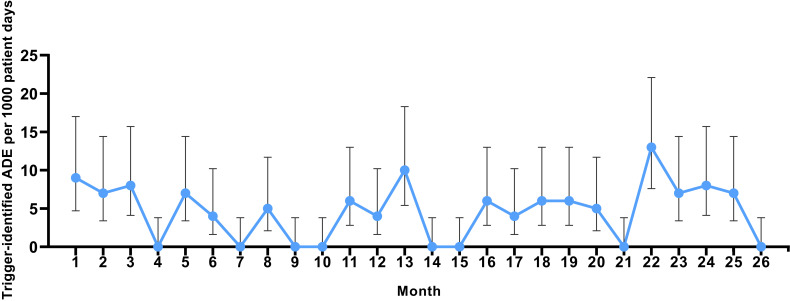
Results: In the development phase, 189 (19%) patients had ≥1 ADE (total 277 ADEs). The time needed to identify these ADEs was 15 minutes/chart. A total of 203 patients had ≥1 trigger (total 273 triggers - Tool B). The sensitivities and specificities of Tools A and B were 0.41 and 0.86, and 0.43 and 0.86, respectively. Tool A was more time-efficient than Tool B (4 vs 9 minutes/chart) and was therefore used in the implementation phase. During the 26-month implementation phase, 22 patients experienced trigger-identified ADEs and 529 did not. The median number of ADEs per 1000 patient days was 6 (range 0-13). Patients with at least one ADE had a mean hospital stay of 22.3 ± 19.7 days, compared to 8.0 ± 7.6 days for those without an ADE (p = 2.7×10-14).
Conclusion: We developed and implemented an e-trigger tool that was specific and moderately sensitive, gave consistent results and required minimal resources.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
