Liyong Lin, Paige A Taylor, Jiajian Shen, Jatinder Saini, Minglei Kang, Charles B Simone, Jeffrey D Bradley, Zuofeng Li, Ying Xiao
{"title":"美国质子治疗中心使用蒙特卡罗剂量计算的NRG肿瘤学调查。","authors":"Liyong Lin, Paige A Taylor, Jiajian Shen, Jatinder Saini, Minglei Kang, Charles B Simone, Jeffrey D Bradley, Zuofeng Li, Ying Xiao","doi":"10.14338/IJPT-D-21-00004","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose/objectives: </strong>Monte Carlo (MC) dose calculation has appeared in primary commercial treatment-planning systems and various in-house platforms. Dual-energy computed tomography (DECT) and metal artifact reduction (MAR) techniques complement MC capabilities. However, no publications have yet reported how proton therapy centers implement these new technologies, and a national survey is required to determine the feasibility of including MC and companion techniques in cooperative group clinical trials.</p><p><strong>Materials/methods: </strong>A 9-question survey was designed to query key clinical parameters: scope of MC utilization, validation methods for heterogeneities, clinical site-specific imaging guidance, proton range uncertainties, and how implants are handled. A national survey was distributed to all 29 operational US proton therapy centers on 13 May 2019.</p><p><strong>Results: </strong>We received responses from 25 centers (86% participation). Commercial MC was most commonly used for primary plan optimization (16 centers) or primary dose evaluation (18 centers), while in-house MC was used more frequently for secondary dose evaluation (7 centers). Based on the survey, MC was used infrequently for gastrointestinal, genitourinary, gynecology and extremity compared with other more heterogeneous disease sites (<i>P</i> < .007). Although many centers had published DECT research, only 3/25 centers had implemented DECT clinically, either in the treatment-planning system or to override implant materials. Most centers (64%) treated patients with metal implants on a case-by-case basis, with a variety of methods reported. Twenty-four centers (96%) used MAR images and overrode the surrounding tissue artifacts; however, there was no consensus on how to determine metal dimension, materials density, or stopping powers.</p><p><strong>Conclusion: </strong>The use of MC for primary dose calculation and optimization was prevalent and, therefore, likely feasible for clinical trials. There was consensus to use MAR and override tissues surrounding metals but no consensus about how to use DECT and MAR for human tissues and implants. Development and standardization of these advanced technologies are strongly encouraged for vendors and clinical physicists.</p>","PeriodicalId":36923,"journal":{"name":"International Journal of Particle Therapy","volume":"8 2","pages":"73-81"},"PeriodicalIF":2.0000,"publicationDate":"2021-05-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8489489/pdf/","citationCount":"6","resultStr":"{\"title\":\"NRG Oncology Survey of Monte Carlo Dose Calculation Use in US Proton Therapy Centers.\",\"authors\":\"Liyong Lin, Paige A Taylor, Jiajian Shen, Jatinder Saini, Minglei Kang, Charles B Simone, Jeffrey D Bradley, Zuofeng Li, Ying Xiao\",\"doi\":\"10.14338/IJPT-D-21-00004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose/objectives: </strong>Monte Carlo (MC) dose calculation has appeared in primary commercial treatment-planning systems and various in-house platforms. Dual-energy computed tomography (DECT) and metal artifact reduction (MAR) techniques complement MC capabilities. However, no publications have yet reported how proton therapy centers implement these new technologies, and a national survey is required to determine the feasibility of including MC and companion techniques in cooperative group clinical trials.</p><p><strong>Materials/methods: </strong>A 9-question survey was designed to query key clinical parameters: scope of MC utilization, validation methods for heterogeneities, clinical site-specific imaging guidance, proton range uncertainties, and how implants are handled. A national survey was distributed to all 29 operational US proton therapy centers on 13 May 2019.</p><p><strong>Results: </strong>We received responses from 25 centers (86% participation). Commercial MC was most commonly used for primary plan optimization (16 centers) or primary dose evaluation (18 centers), while in-house MC was used more frequently for secondary dose evaluation (7 centers). Based on the survey, MC was used infrequently for gastrointestinal, genitourinary, gynecology and extremity compared with other more heterogeneous disease sites (<i>P</i> < .007). Although many centers had published DECT research, only 3/25 centers had implemented DECT clinically, either in the treatment-planning system or to override implant materials. Most centers (64%) treated patients with metal implants on a case-by-case basis, with a variety of methods reported. Twenty-four centers (96%) used MAR images and overrode the surrounding tissue artifacts; however, there was no consensus on how to determine metal dimension, materials density, or stopping powers.</p><p><strong>Conclusion: </strong>The use of MC for primary dose calculation and optimization was prevalent and, therefore, likely feasible for clinical trials. There was consensus to use MAR and override tissues surrounding metals but no consensus about how to use DECT and MAR for human tissues and implants. Development and standardization of these advanced technologies are strongly encouraged for vendors and clinical physicists.</p>\",\"PeriodicalId\":36923,\"journal\":{\"name\":\"International Journal of Particle Therapy\",\"volume\":\"8 2\",\"pages\":\"73-81\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2021-05-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8489489/pdf/\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Particle Therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14338/IJPT-D-21-00004\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Particle Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14338/IJPT-D-21-00004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
NRG Oncology Survey of Monte Carlo Dose Calculation Use in US Proton Therapy Centers.
Purpose/objectives: Monte Carlo (MC) dose calculation has appeared in primary commercial treatment-planning systems and various in-house platforms. Dual-energy computed tomography (DECT) and metal artifact reduction (MAR) techniques complement MC capabilities. However, no publications have yet reported how proton therapy centers implement these new technologies, and a national survey is required to determine the feasibility of including MC and companion techniques in cooperative group clinical trials.
Materials/methods: A 9-question survey was designed to query key clinical parameters: scope of MC utilization, validation methods for heterogeneities, clinical site-specific imaging guidance, proton range uncertainties, and how implants are handled. A national survey was distributed to all 29 operational US proton therapy centers on 13 May 2019.
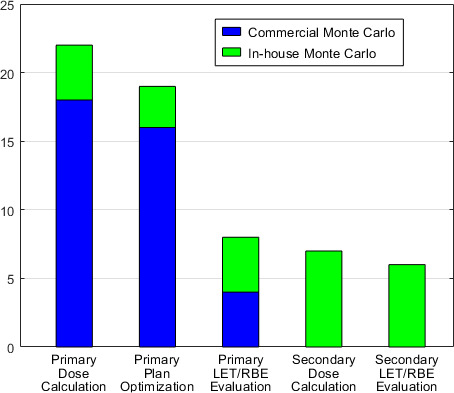
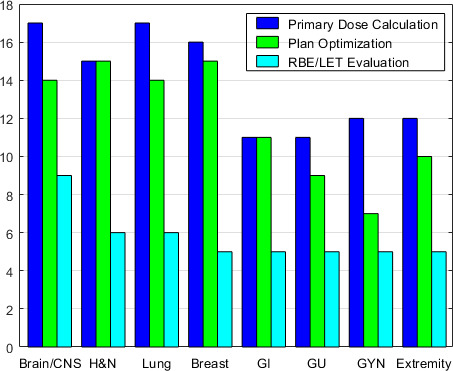
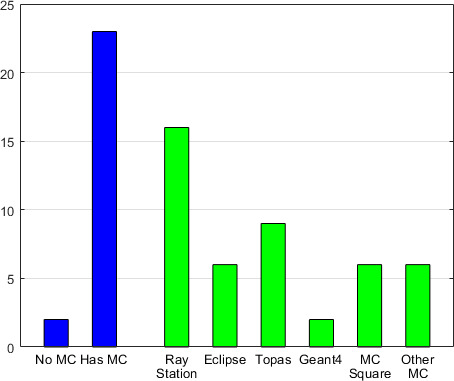
Results: We received responses from 25 centers (86% participation). Commercial MC was most commonly used for primary plan optimization (16 centers) or primary dose evaluation (18 centers), while in-house MC was used more frequently for secondary dose evaluation (7 centers). Based on the survey, MC was used infrequently for gastrointestinal, genitourinary, gynecology and extremity compared with other more heterogeneous disease sites (P < .007). Although many centers had published DECT research, only 3/25 centers had implemented DECT clinically, either in the treatment-planning system or to override implant materials. Most centers (64%) treated patients with metal implants on a case-by-case basis, with a variety of methods reported. Twenty-four centers (96%) used MAR images and overrode the surrounding tissue artifacts; however, there was no consensus on how to determine metal dimension, materials density, or stopping powers.
Conclusion: The use of MC for primary dose calculation and optimization was prevalent and, therefore, likely feasible for clinical trials. There was consensus to use MAR and override tissues surrounding metals but no consensus about how to use DECT and MAR for human tissues and implants. Development and standardization of these advanced technologies are strongly encouraged for vendors and clinical physicists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
