Yuan Shao, Yuyun Xu, Yumei Li, Xuehua Wen, Xiaodong He
{"title":"介入后脑高密度新分类系统:对急性脑卒中出血转化及临床预后的影响。","authors":"Yuan Shao, Yuyun Xu, Yumei Li, Xuehua Wen, Xiaodong He","doi":"10.1155/2021/6144304","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postinterventional cerebral hyperdensity (PCHD) is commonly seen in acute ischemic patients after mechanical thrombectomy. We propose a new classification of PCHD to investigate its correlation with hemorrhagic transformation (HT). The clinical prognosis of PCHD was further studied.</p><p><strong>Methods: </strong>Data from 189 acute stroke patients were analyzed retrospectively. According to the European Cooperative Acute Stroke Study criteria (ECASS), HT was classified as hemorrhagic infarction (HI-1 and HI-2) and parenchymal hematoma (pH-1 and pH-2). Referring to the classification of HT, PCHD was classified as PCHD-1, PCHD-2, PCHD-3, and PCHD-4. The prognosis included early neurological deterioration (END) and the modified Rankin Scale (mRS) score at 3 months.</p><p><strong>Results: </strong>The incidence of HT was 14.8% (12/81) in the no-PCHD group and 77.8% (84/108) in the PCHD group. PCHD was highly correlated with HT (<i>r</i> = 0.751, <i>p</i> < 0.01). After stepwise regression analysis, PCHD and the National Institutes of Health Stroke Scale (NIHSS) score at admission were found to be independent factors for END (<i>p</i> < 0.001, <i>p</i> = 0.015, respectively). The area of curves (AUC) of PCHD, the NIHSS at admission, and the combined model were 0.810, 0.667, and 0.832, respectively. The optimal diagnostic cutoff of PCHD for END was PCHD > 2. PCHD, the NIHSS score at admission, and good vascular recanalization (VR) were independently associated with 3-month mRS (all <i>p</i> < 0.05). The AUC of PCHD, the NIHSS at admission, good VR, and the combined model were 0.779, 0.733, 0.565, and 0.867, respectively. And the best cutoff of PCHD for the mRS was PCHD > 1.</p><p><strong>Conclusion: </strong>The relationship of PCHD and HT suggested PCHD was an early risk indicator for HT. The occurrence of PCHD-3 and PCHD-4 was a strong predictor for END. PCHD-1 is considered to be relatively benign in relation to the 3-month mRS.</p>","PeriodicalId":51299,"journal":{"name":"Neural Plasticity","volume":" ","pages":"6144304"},"PeriodicalIF":3.7000,"publicationDate":"2021-11-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8632469/pdf/","citationCount":"0","resultStr":"{\"title\":\"A New Classification System for Postinterventional Cerebral Hyperdensity: The Influence on Hemorrhagic Transformation and Clinical Prognosis in Acute Stroke.\",\"authors\":\"Yuan Shao, Yuyun Xu, Yumei Li, Xuehua Wen, Xiaodong He\",\"doi\":\"10.1155/2021/6144304\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Postinterventional cerebral hyperdensity (PCHD) is commonly seen in acute ischemic patients after mechanical thrombectomy. We propose a new classification of PCHD to investigate its correlation with hemorrhagic transformation (HT). The clinical prognosis of PCHD was further studied.</p><p><strong>Methods: </strong>Data from 189 acute stroke patients were analyzed retrospectively. According to the European Cooperative Acute Stroke Study criteria (ECASS), HT was classified as hemorrhagic infarction (HI-1 and HI-2) and parenchymal hematoma (pH-1 and pH-2). Referring to the classification of HT, PCHD was classified as PCHD-1, PCHD-2, PCHD-3, and PCHD-4. The prognosis included early neurological deterioration (END) and the modified Rankin Scale (mRS) score at 3 months.</p><p><strong>Results: </strong>The incidence of HT was 14.8% (12/81) in the no-PCHD group and 77.8% (84/108) in the PCHD group. PCHD was highly correlated with HT (<i>r</i> = 0.751, <i>p</i> < 0.01). After stepwise regression analysis, PCHD and the National Institutes of Health Stroke Scale (NIHSS) score at admission were found to be independent factors for END (<i>p</i> < 0.001, <i>p</i> = 0.015, respectively). The area of curves (AUC) of PCHD, the NIHSS at admission, and the combined model were 0.810, 0.667, and 0.832, respectively. The optimal diagnostic cutoff of PCHD for END was PCHD > 2. PCHD, the NIHSS score at admission, and good vascular recanalization (VR) were independently associated with 3-month mRS (all <i>p</i> < 0.05). The AUC of PCHD, the NIHSS at admission, good VR, and the combined model were 0.779, 0.733, 0.565, and 0.867, respectively. And the best cutoff of PCHD for the mRS was PCHD > 1.</p><p><strong>Conclusion: </strong>The relationship of PCHD and HT suggested PCHD was an early risk indicator for HT. The occurrence of PCHD-3 and PCHD-4 was a strong predictor for END. PCHD-1 is considered to be relatively benign in relation to the 3-month mRS.</p>\",\"PeriodicalId\":51299,\"journal\":{\"name\":\"Neural Plasticity\",\"volume\":\" \",\"pages\":\"6144304\"},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2021-11-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8632469/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neural Plasticity\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2021/6144304\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"NEUROSCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neural Plasticity","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2021/6144304","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
引用次数: 0
摘要
背景:介入后脑高密度(PCHD)常见于机械取栓术后急性缺血性患者。我们提出一种新的PCHD分类,以探讨其与出血性转化(HT)的关系。进一步研究PCHD的临床预后。方法:回顾性分析189例急性脑卒中患者的资料。根据欧洲急性卒中合作研究标准(ECASS), HT分为出血性梗死(HI-1和HI-2)和实质血肿(pH-1和pH-2)。参照HT的分类,将PCHD分为PCHD-1、PCHD-2、PCHD-3、PCHD-4。预后包括早期神经功能恶化(END)和3个月时的改良Rankin量表(mRS)评分。结果:无PCHD组HT发生率为14.8% (12/81),PCHD组为77.8%(84/108)。PCHD与HT高度相关(r = 0.751, p < 0.01)。逐步回归分析发现入院时PCHD和NIHSS评分是影响END的独立因素(p < 0.001, p = 0.015)。入院时PCHD、NIHSS曲线面积(AUC)和联合模型分别为0.810、0.667和0.832。PCHD诊断END的最佳临界值为PCHD > 2。PCHD、入院时NIHSS评分、良好血管再通(VR)与3个月mRS独立相关(均p < 0.05)。PCHD、入院时NIHSS、良好VR和综合模型的AUC分别为0.779、0.733、0.565和0.867。PCHD的最佳临界值为PCHD > 1。结论:PCHD与HT的关系提示PCHD是HT的早期危险指标。PCHD-3和PCHD-4的出现是END的重要预测因子。与3个月的mRS相比,PCHD-1被认为是相对良性的。
A New Classification System for Postinterventional Cerebral Hyperdensity: The Influence on Hemorrhagic Transformation and Clinical Prognosis in Acute Stroke.
Background: Postinterventional cerebral hyperdensity (PCHD) is commonly seen in acute ischemic patients after mechanical thrombectomy. We propose a new classification of PCHD to investigate its correlation with hemorrhagic transformation (HT). The clinical prognosis of PCHD was further studied.
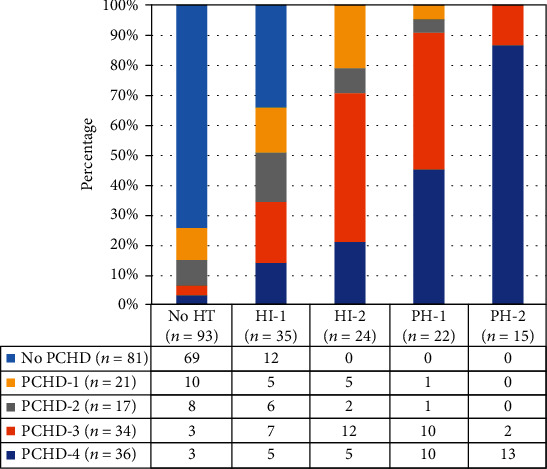
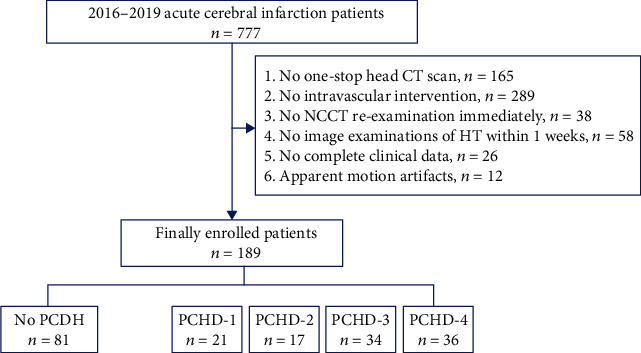
Methods: Data from 189 acute stroke patients were analyzed retrospectively. According to the European Cooperative Acute Stroke Study criteria (ECASS), HT was classified as hemorrhagic infarction (HI-1 and HI-2) and parenchymal hematoma (pH-1 and pH-2). Referring to the classification of HT, PCHD was classified as PCHD-1, PCHD-2, PCHD-3, and PCHD-4. The prognosis included early neurological deterioration (END) and the modified Rankin Scale (mRS) score at 3 months.
Results: The incidence of HT was 14.8% (12/81) in the no-PCHD group and 77.8% (84/108) in the PCHD group. PCHD was highly correlated with HT (r = 0.751, p < 0.01). After stepwise regression analysis, PCHD and the National Institutes of Health Stroke Scale (NIHSS) score at admission were found to be independent factors for END (p < 0.001, p = 0.015, respectively). The area of curves (AUC) of PCHD, the NIHSS at admission, and the combined model were 0.810, 0.667, and 0.832, respectively. The optimal diagnostic cutoff of PCHD for END was PCHD > 2. PCHD, the NIHSS score at admission, and good vascular recanalization (VR) were independently associated with 3-month mRS (all p < 0.05). The AUC of PCHD, the NIHSS at admission, good VR, and the combined model were 0.779, 0.733, 0.565, and 0.867, respectively. And the best cutoff of PCHD for the mRS was PCHD > 1.
Conclusion: The relationship of PCHD and HT suggested PCHD was an early risk indicator for HT. The occurrence of PCHD-3 and PCHD-4 was a strong predictor for END. PCHD-1 is considered to be relatively benign in relation to the 3-month mRS.
期刊介绍:
Neural Plasticity is an international, interdisciplinary journal dedicated to the publication of articles related to all aspects of neural plasticity, with special emphasis on its functional significance as reflected in behavior and in psychopathology. Neural Plasticity publishes research and review articles from the entire range of relevant disciplines, including basic neuroscience, behavioral neuroscience, cognitive neuroscience, biological psychology, and biological psychiatry.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
