Tufan Çınar, Suha Asal, Vedat Çiçek, Murat Selçuk, Muhammed Keskin, Ahmet Lütfullah Orhan
{"title":"急性髂外动脉闭塞是冠状动脉造影中一种罕见的并发症。","authors":"Tufan Çınar, Suha Asal, Vedat Çiçek, Murat Selçuk, Muhammed Keskin, Ahmet Lütfullah Orhan","doi":"10.18502/jthc.v16i1.6603","DOIUrl":null,"url":null,"abstract":"<p><p>A 40-year-old female patient presented to our cardiology department with typical angina of 1 month's duration. The patient was on a combination of valsartan and hydrochlorothiazide for the treatment of hypertension. Electrocardiography showed a normal sinus rhythm with T-wave negativity in the anterior precordial leads. A cardiovascular stress test with the Bruce protocol revealed 2 mm horizontal ST-segment deviation in the inferior and lateral leads. Therefore, the patient was scheduled to undergo coronary angiography (CAG). Before CAG, she was anxious and stressed; hence, intravenous diazepam was administered. CAG, performed via the right femoral artery, demonstrated an insignificant muscular bridge in the mid-portion of the left anterior descending artery (Figure 1A). Twenty minutes after the procedure, the patient felt numbness in her right lower leg and had difficulties in her movements. On physical examination, there was no pulse in the right lower extremity. Because of the presence of the signs and symptoms of acute lower extremity ischemia, an urgent peripheral angiography via the left femoral artery was performed. It illustrated an acute occlusion in the external iliac artery (EIA) (Figure 1B and Video 1). Afterward, intravenous nitroglycerin and unfractionated heparin (5000 U) were given through the right diagnostic catheter. Following this therapy, antegrade blood flow was achieved in the EIA and the signs and symptoms of acute limb ischemia disappeared (Figure 1C and Video 2). Arterial duplex ultrasonography just after this procedure revealed a retrograde arterial dissection flap without significant stenosis (Figure 1D-E and Video 3). In addition, a triphasic blood-flow pattern was observed in the EIA (Figure 1E). During coronary intensive care, intravenous low-dose nitroglycerin and unfractionated heparin were administered for 48 hours. The in-hospital follow-up of the patient was uneventful, and there were no signs and symptoms of peripheral embolism. Arterial duplex ultrasonography, performed 2 weeks after hospital discharge, showed that there was no residual stenosis and that the dissection flap was sealed. Arterial dissection is an infrequent clinical entity encountered during CAG. Remarkably, even though vasospasm and compression to the access site were other contributing factors, acute EIA occlusion due to retrograde dissection is an extremely rare event. As was shown in our case, medical therapy, including intravenous nitroglycerin and unfractionated heparin, could potentially allow the resolution of the total occlusion of the EIA without necessitating percutaneous transluminal angioplasty or stenting.</p>","PeriodicalId":39149,"journal":{"name":"Journal of Tehran University Heart Center","volume":"16 1","pages":"45-46"},"PeriodicalIF":0.0000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/18/JTHC-16-45.PMC8728861.pdf","citationCount":"1","resultStr":"{\"title\":\"Acute External Iliac Artery Occlusion as an Uncommon Complication Encountered during Coronary Angiography.\",\"authors\":\"Tufan Çınar, Suha Asal, Vedat Çiçek, Murat Selçuk, Muhammed Keskin, Ahmet Lütfullah Orhan\",\"doi\":\"10.18502/jthc.v16i1.6603\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 40-year-old female patient presented to our cardiology department with typical angina of 1 month's duration. The patient was on a combination of valsartan and hydrochlorothiazide for the treatment of hypertension. Electrocardiography showed a normal sinus rhythm with T-wave negativity in the anterior precordial leads. A cardiovascular stress test with the Bruce protocol revealed 2 mm horizontal ST-segment deviation in the inferior and lateral leads. Therefore, the patient was scheduled to undergo coronary angiography (CAG). Before CAG, she was anxious and stressed; hence, intravenous diazepam was administered. CAG, performed via the right femoral artery, demonstrated an insignificant muscular bridge in the mid-portion of the left anterior descending artery (Figure 1A). Twenty minutes after the procedure, the patient felt numbness in her right lower leg and had difficulties in her movements. On physical examination, there was no pulse in the right lower extremity. Because of the presence of the signs and symptoms of acute lower extremity ischemia, an urgent peripheral angiography via the left femoral artery was performed. It illustrated an acute occlusion in the external iliac artery (EIA) (Figure 1B and Video 1). Afterward, intravenous nitroglycerin and unfractionated heparin (5000 U) were given through the right diagnostic catheter. Following this therapy, antegrade blood flow was achieved in the EIA and the signs and symptoms of acute limb ischemia disappeared (Figure 1C and Video 2). Arterial duplex ultrasonography just after this procedure revealed a retrograde arterial dissection flap without significant stenosis (Figure 1D-E and Video 3). In addition, a triphasic blood-flow pattern was observed in the EIA (Figure 1E). During coronary intensive care, intravenous low-dose nitroglycerin and unfractionated heparin were administered for 48 hours. The in-hospital follow-up of the patient was uneventful, and there were no signs and symptoms of peripheral embolism. Arterial duplex ultrasonography, performed 2 weeks after hospital discharge, showed that there was no residual stenosis and that the dissection flap was sealed. Arterial dissection is an infrequent clinical entity encountered during CAG. Remarkably, even though vasospasm and compression to the access site were other contributing factors, acute EIA occlusion due to retrograde dissection is an extremely rare event. As was shown in our case, medical therapy, including intravenous nitroglycerin and unfractionated heparin, could potentially allow the resolution of the total occlusion of the EIA without necessitating percutaneous transluminal angioplasty or stenting.</p>\",\"PeriodicalId\":39149,\"journal\":{\"name\":\"Journal of Tehran University Heart Center\",\"volume\":\"16 1\",\"pages\":\"45-46\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/18/JTHC-16-45.PMC8728861.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Tehran University Heart Center\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.18502/jthc.v16i1.6603\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Tehran University Heart Center","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jthc.v16i1.6603","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Acute External Iliac Artery Occlusion as an Uncommon Complication Encountered during Coronary Angiography.
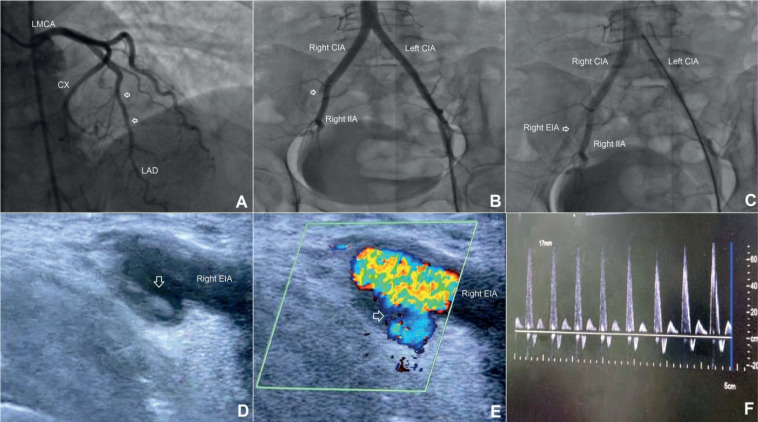
A 40-year-old female patient presented to our cardiology department with typical angina of 1 month's duration. The patient was on a combination of valsartan and hydrochlorothiazide for the treatment of hypertension. Electrocardiography showed a normal sinus rhythm with T-wave negativity in the anterior precordial leads. A cardiovascular stress test with the Bruce protocol revealed 2 mm horizontal ST-segment deviation in the inferior and lateral leads. Therefore, the patient was scheduled to undergo coronary angiography (CAG). Before CAG, she was anxious and stressed; hence, intravenous diazepam was administered. CAG, performed via the right femoral artery, demonstrated an insignificant muscular bridge in the mid-portion of the left anterior descending artery (Figure 1A). Twenty minutes after the procedure, the patient felt numbness in her right lower leg and had difficulties in her movements. On physical examination, there was no pulse in the right lower extremity. Because of the presence of the signs and symptoms of acute lower extremity ischemia, an urgent peripheral angiography via the left femoral artery was performed. It illustrated an acute occlusion in the external iliac artery (EIA) (Figure 1B and Video 1). Afterward, intravenous nitroglycerin and unfractionated heparin (5000 U) were given through the right diagnostic catheter. Following this therapy, antegrade blood flow was achieved in the EIA and the signs and symptoms of acute limb ischemia disappeared (Figure 1C and Video 2). Arterial duplex ultrasonography just after this procedure revealed a retrograde arterial dissection flap without significant stenosis (Figure 1D-E and Video 3). In addition, a triphasic blood-flow pattern was observed in the EIA (Figure 1E). During coronary intensive care, intravenous low-dose nitroglycerin and unfractionated heparin were administered for 48 hours. The in-hospital follow-up of the patient was uneventful, and there were no signs and symptoms of peripheral embolism. Arterial duplex ultrasonography, performed 2 weeks after hospital discharge, showed that there was no residual stenosis and that the dissection flap was sealed. Arterial dissection is an infrequent clinical entity encountered during CAG. Remarkably, even though vasospasm and compression to the access site were other contributing factors, acute EIA occlusion due to retrograde dissection is an extremely rare event. As was shown in our case, medical therapy, including intravenous nitroglycerin and unfractionated heparin, could potentially allow the resolution of the total occlusion of the EIA without necessitating percutaneous transluminal angioplasty or stenting.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
