{"title":"交通性支气管肺前肠畸形IB型:诊断和手术挑战。","authors":"Bhushanrao Jadhav, Ranjithatharsini Vaseeharan, Prabhu Sekaran, Semiu Eniola Folaranmi, Karim Awad","doi":"10.1055/s-0041-1740321","DOIUrl":null,"url":null,"abstract":"<p><p>Communicating bronchopulmonary foregut malformations (CBPFM) are extremely rare. We present a complex case of type IB CBPFM with esophageal atresia and distal tracheoesophageal fistula (EA/TOF), duodenal atresia/annular pancreas (DA/AP), and intestinal malrotation who underwent primary repair for EA/TOF on day 3. Bilious aspirates on day 8 prompted an upper gastrointestinal (GI) contrast revealing a duodenal obstruction and communication between the right lung lower lobe and the esophagus (T8-T9 level). DA/AP and malrotation were repaired by a gastrojejunostomy and Ladd's procedure. A repeat contrast swallow identified a 2nd communication from the esophagus into the right lower lobe (T5-T6 level) raising the suspicion of a recurrent TOF. Computed tomography (CT) thorax confirmed above findings with an anomalous blood supply to right lung. An exploratory thoracotomy identified a three-lobed lung. However, the lower lobe was enlarged and connected in two separate locations to the esophagus. The child recovered after the disconnection of the esophageal connections and partial right lower lobectomy. CBPFM are extremely rare anomalies requiring a high index of suspicion, use of an upper GI contrast series, and CT scans for diagnosis. The treatment of choice is resection of the affected lung and disconnection of the esophageal communications.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":"9 1","pages":"e80-e83"},"PeriodicalIF":0.7000,"publicationDate":"2021-12-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8668381/pdf/","citationCount":"3","resultStr":"{\"title\":\"Communicating Bronchopulmonary Foregut Malformation Type IB: Diagnostic and Surgical Challenges.\",\"authors\":\"Bhushanrao Jadhav, Ranjithatharsini Vaseeharan, Prabhu Sekaran, Semiu Eniola Folaranmi, Karim Awad\",\"doi\":\"10.1055/s-0041-1740321\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Communicating bronchopulmonary foregut malformations (CBPFM) are extremely rare. We present a complex case of type IB CBPFM with esophageal atresia and distal tracheoesophageal fistula (EA/TOF), duodenal atresia/annular pancreas (DA/AP), and intestinal malrotation who underwent primary repair for EA/TOF on day 3. Bilious aspirates on day 8 prompted an upper gastrointestinal (GI) contrast revealing a duodenal obstruction and communication between the right lung lower lobe and the esophagus (T8-T9 level). DA/AP and malrotation were repaired by a gastrojejunostomy and Ladd's procedure. A repeat contrast swallow identified a 2nd communication from the esophagus into the right lower lobe (T5-T6 level) raising the suspicion of a recurrent TOF. Computed tomography (CT) thorax confirmed above findings with an anomalous blood supply to right lung. An exploratory thoracotomy identified a three-lobed lung. However, the lower lobe was enlarged and connected in two separate locations to the esophagus. The child recovered after the disconnection of the esophageal connections and partial right lower lobectomy. CBPFM are extremely rare anomalies requiring a high index of suspicion, use of an upper GI contrast series, and CT scans for diagnosis. The treatment of choice is resection of the affected lung and disconnection of the esophageal communications.</p>\",\"PeriodicalId\":43204,\"journal\":{\"name\":\"European Journal of Pediatric Surgery Reports\",\"volume\":\"9 1\",\"pages\":\"e80-e83\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2021-12-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8668381/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Pediatric Surgery Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0041-1740321\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0041-1740321","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Communicating Bronchopulmonary Foregut Malformation Type IB: Diagnostic and Surgical Challenges.
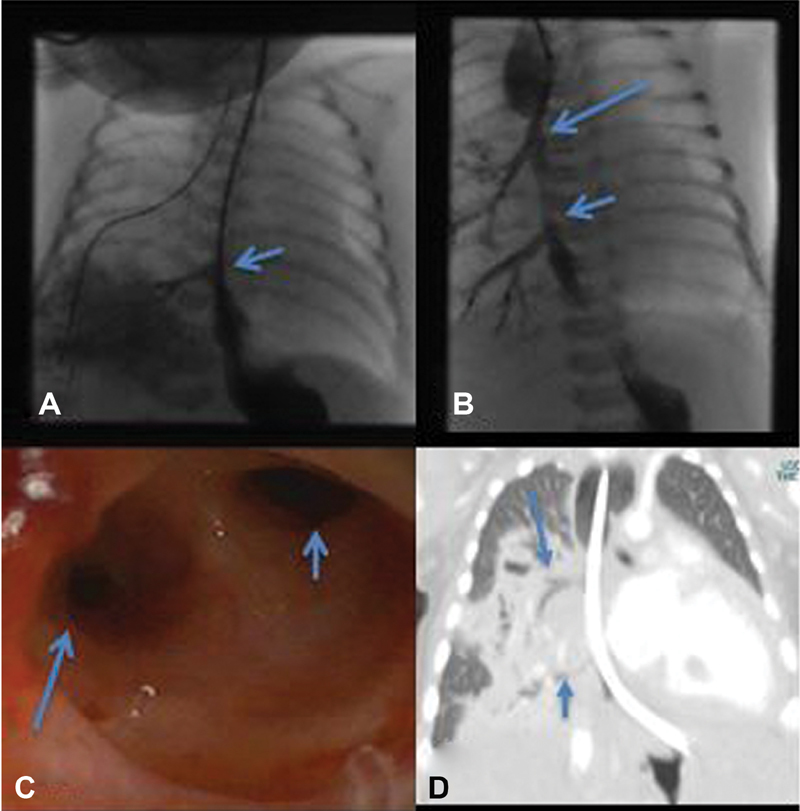
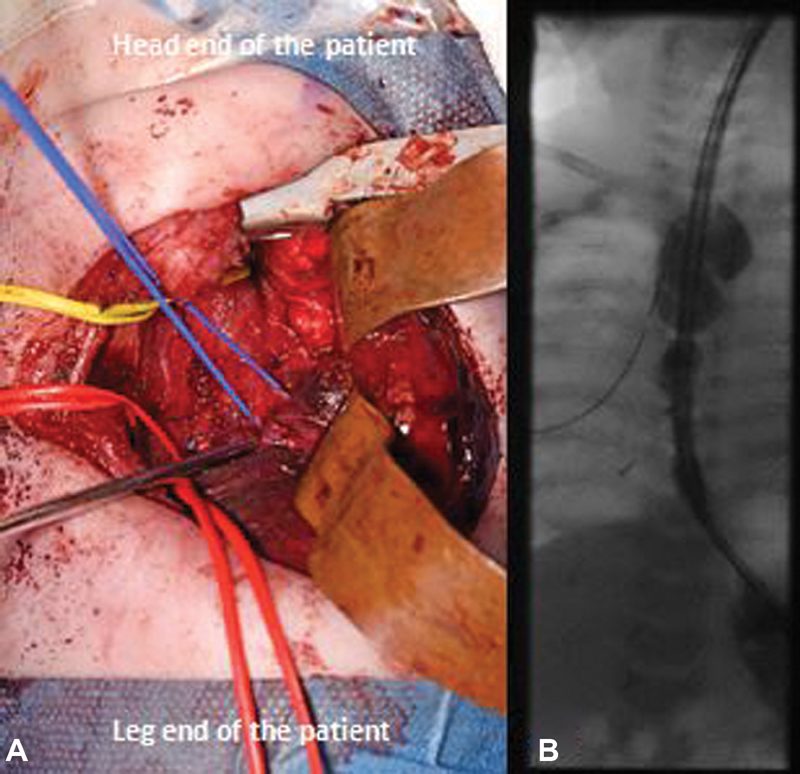
Communicating bronchopulmonary foregut malformations (CBPFM) are extremely rare. We present a complex case of type IB CBPFM with esophageal atresia and distal tracheoesophageal fistula (EA/TOF), duodenal atresia/annular pancreas (DA/AP), and intestinal malrotation who underwent primary repair for EA/TOF on day 3. Bilious aspirates on day 8 prompted an upper gastrointestinal (GI) contrast revealing a duodenal obstruction and communication between the right lung lower lobe and the esophagus (T8-T9 level). DA/AP and malrotation were repaired by a gastrojejunostomy and Ladd's procedure. A repeat contrast swallow identified a 2nd communication from the esophagus into the right lower lobe (T5-T6 level) raising the suspicion of a recurrent TOF. Computed tomography (CT) thorax confirmed above findings with an anomalous blood supply to right lung. An exploratory thoracotomy identified a three-lobed lung. However, the lower lobe was enlarged and connected in two separate locations to the esophagus. The child recovered after the disconnection of the esophageal connections and partial right lower lobectomy. CBPFM are extremely rare anomalies requiring a high index of suspicion, use of an upper GI contrast series, and CT scans for diagnosis. The treatment of choice is resection of the affected lung and disconnection of the esophageal communications.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
