Philip Dueppers, Lorenz Meuli, Benedikt Reutersberg, Michael Hofmann, Florian Messmer, Alexander Zimmermann
{"title":"胸主动脉疾病左锁骨下动脉切开与血管内分离的早期和中期结果","authors":"Philip Dueppers, Lorenz Meuli, Benedikt Reutersberg, Michael Hofmann, Florian Messmer, Alexander Zimmermann","doi":"10.5761/atcs.oa.21-00206","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To compare open versus endovascular left subclavian artery debranching for thoracic endovascular aortic repair of thoracic aortic pathologies.</p><p><strong>Methods: </strong>This is a retrospective study of patients receiving left subclavian artery debranching in our institution from October 2009 to January 2020. The primary outcome was freedom from aortic reintervention. Secondary outcomes were type I endoleaks, left subclavian artery (LSA) debranching failure, stroke, technical or clinical success, procedure-related reintervention, as well as 30-day or overall all-cause and aorta-related mortality.</p><p><strong>Results: </strong>Forty-eight patients received parallel graft-based (n = 24, ENDO; median age 75 years [70-80 years]) or open (n = 24, OPEN; median age 71 years [59-75 years]) debranching for type B aortic dissection (n = 25), degenerative aneurysm (n = 12), type IA endoleak (n = 6), suture-associated (n = 3) or ostial LSA aneurysm (n = 1), or penetrating aortic ulcer (n = 1). The median follow-up was 36 months (13-61 months). After 16 months, aortic reintervention-free survival in groups OPEN and ENDO was 91% (95% confidence interval [CI]: 79 to 100%) and 86% (73 to 100%) (p = 0.71), respectively. After 36 months, all-cause survival in groups OPEN and ENDO was 74% (95% CI: 55 to 99%) and 79% (95% CI: 64 to 97%) (p = 0.74), respectively; freedom from aorta-related mortality was 81% (95% CI: 62 to 100%) and 91% (95% CI: 80 to 100%) (p = 0.78), respectively. Group OPEN presented less type I endoleaks (OPEN/ENDO = 3/19, p <0.001) and higher technical (OPEN/ENDO = 81/36%, p = 0.003) and clinical success rates (OPEN/ENDO = 67/36%, p = 0.047). No statistical differences were found for other outcomes.</p><p><strong>Conclusion: </strong>Both strategies achieved comparable reintervention and mortality rates, but open debranching should be preferred due to its higher technical and clinical success and less type I endoleaks.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":"28 3","pages":"193-203"},"PeriodicalIF":1.3000,"publicationDate":"2022-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cf/d0/atcs-28-193.PMC9209886.pdf","citationCount":"5","resultStr":"{\"title\":\"Early and Mid-Term Outcomes of Open versus Endovascular Left Subclavian Artery Debranching for Thoracic Aortic Diseases.\",\"authors\":\"Philip Dueppers, Lorenz Meuli, Benedikt Reutersberg, Michael Hofmann, Florian Messmer, Alexander Zimmermann\",\"doi\":\"10.5761/atcs.oa.21-00206\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To compare open versus endovascular left subclavian artery debranching for thoracic endovascular aortic repair of thoracic aortic pathologies.</p><p><strong>Methods: </strong>This is a retrospective study of patients receiving left subclavian artery debranching in our institution from October 2009 to January 2020. The primary outcome was freedom from aortic reintervention. Secondary outcomes were type I endoleaks, left subclavian artery (LSA) debranching failure, stroke, technical or clinical success, procedure-related reintervention, as well as 30-day or overall all-cause and aorta-related mortality.</p><p><strong>Results: </strong>Forty-eight patients received parallel graft-based (n = 24, ENDO; median age 75 years [70-80 years]) or open (n = 24, OPEN; median age 71 years [59-75 years]) debranching for type B aortic dissection (n = 25), degenerative aneurysm (n = 12), type IA endoleak (n = 6), suture-associated (n = 3) or ostial LSA aneurysm (n = 1), or penetrating aortic ulcer (n = 1). The median follow-up was 36 months (13-61 months). After 16 months, aortic reintervention-free survival in groups OPEN and ENDO was 91% (95% confidence interval [CI]: 79 to 100%) and 86% (73 to 100%) (p = 0.71), respectively. After 36 months, all-cause survival in groups OPEN and ENDO was 74% (95% CI: 55 to 99%) and 79% (95% CI: 64 to 97%) (p = 0.74), respectively; freedom from aorta-related mortality was 81% (95% CI: 62 to 100%) and 91% (95% CI: 80 to 100%) (p = 0.78), respectively. Group OPEN presented less type I endoleaks (OPEN/ENDO = 3/19, p <0.001) and higher technical (OPEN/ENDO = 81/36%, p = 0.003) and clinical success rates (OPEN/ENDO = 67/36%, p = 0.047). No statistical differences were found for other outcomes.</p><p><strong>Conclusion: </strong>Both strategies achieved comparable reintervention and mortality rates, but open debranching should be preferred due to its higher technical and clinical success and less type I endoleaks.</p>\",\"PeriodicalId\":8037,\"journal\":{\"name\":\"Annals of Thoracic and Cardiovascular Surgery\",\"volume\":\"28 3\",\"pages\":\"193-203\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-06-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cf/d0/atcs-28-193.PMC9209886.pdf\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5761/atcs.oa.21-00206\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/12/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.21-00206","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/12/22 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Early and Mid-Term Outcomes of Open versus Endovascular Left Subclavian Artery Debranching for Thoracic Aortic Diseases.
Purpose: To compare open versus endovascular left subclavian artery debranching for thoracic endovascular aortic repair of thoracic aortic pathologies.
Methods: This is a retrospective study of patients receiving left subclavian artery debranching in our institution from October 2009 to January 2020. The primary outcome was freedom from aortic reintervention. Secondary outcomes were type I endoleaks, left subclavian artery (LSA) debranching failure, stroke, technical or clinical success, procedure-related reintervention, as well as 30-day or overall all-cause and aorta-related mortality.
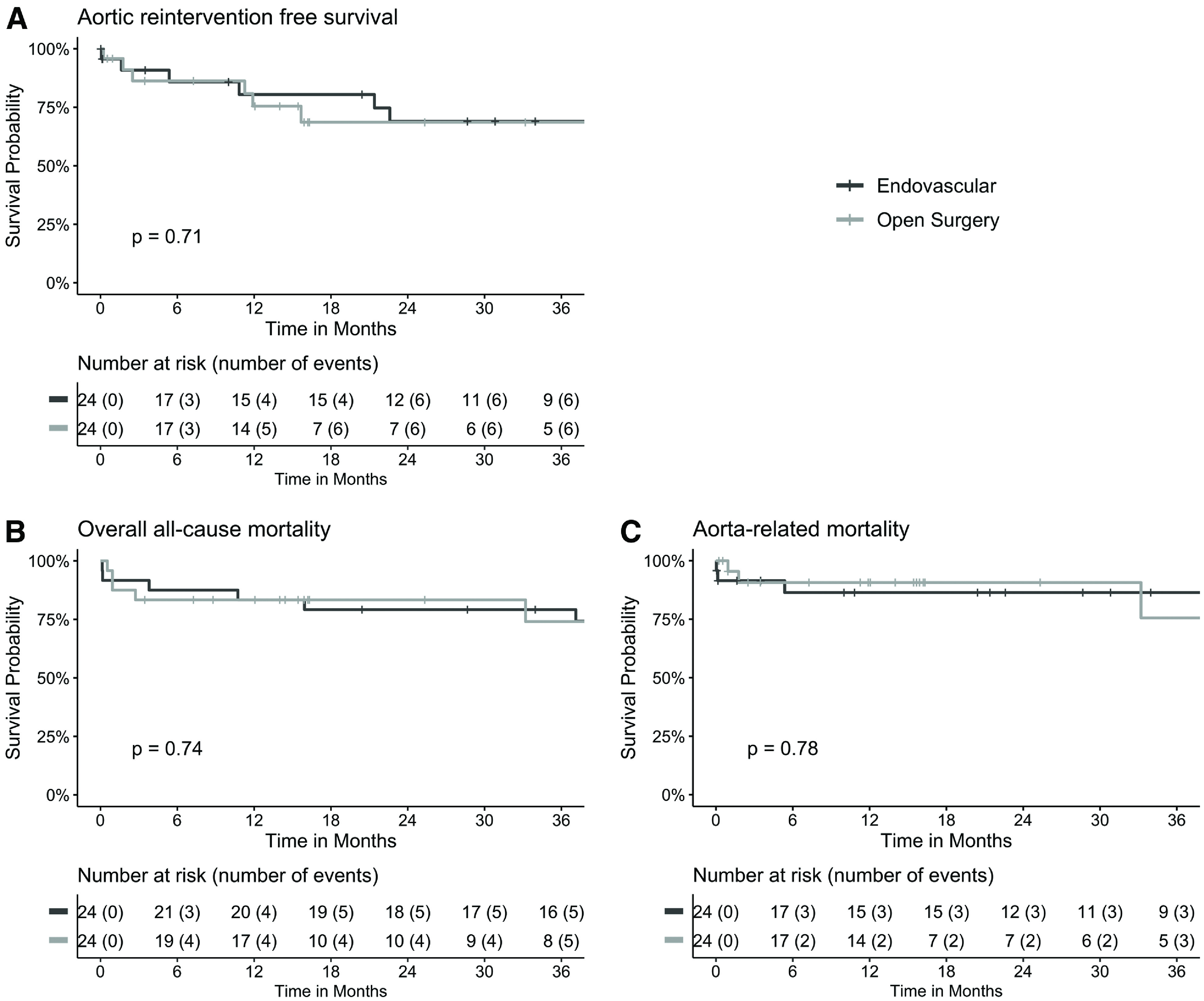
Results: Forty-eight patients received parallel graft-based (n = 24, ENDO; median age 75 years [70-80 years]) or open (n = 24, OPEN; median age 71 years [59-75 years]) debranching for type B aortic dissection (n = 25), degenerative aneurysm (n = 12), type IA endoleak (n = 6), suture-associated (n = 3) or ostial LSA aneurysm (n = 1), or penetrating aortic ulcer (n = 1). The median follow-up was 36 months (13-61 months). After 16 months, aortic reintervention-free survival in groups OPEN and ENDO was 91% (95% confidence interval [CI]: 79 to 100%) and 86% (73 to 100%) (p = 0.71), respectively. After 36 months, all-cause survival in groups OPEN and ENDO was 74% (95% CI: 55 to 99%) and 79% (95% CI: 64 to 97%) (p = 0.74), respectively; freedom from aorta-related mortality was 81% (95% CI: 62 to 100%) and 91% (95% CI: 80 to 100%) (p = 0.78), respectively. Group OPEN presented less type I endoleaks (OPEN/ENDO = 3/19, p <0.001) and higher technical (OPEN/ENDO = 81/36%, p = 0.003) and clinical success rates (OPEN/ENDO = 67/36%, p = 0.047). No statistical differences were found for other outcomes.
Conclusion: Both strategies achieved comparable reintervention and mortality rates, but open debranching should be preferred due to its higher technical and clinical success and less type I endoleaks.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
