Adam Stenman, Magnus Kjellman, Jan Zedenius, C Christofer Juhlin
{"title":"甲状腺乳头状癌和滤泡癌的同步侧淋巴结转移:病例报告和文献复习。","authors":"Adam Stenman, Magnus Kjellman, Jan Zedenius, C Christofer Juhlin","doi":"10.1186/s13044-022-00120-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Follicular thyroid carcinomas (FTCs) rarely metastasize to regional lymph nodes, and descriptions of synchronous lateral lymph node metastases of FTC and papillary thyroid carcinoma (PTC) are lacking.</p><p><strong>Case presentation: </strong>We describe a 43-year-old female with a preoperative cytology indicating a right-sided PTC with lateral lymph node metastases. She underwent a total thyroidectomy and central and lateral lymph node dissection, and histopathology confirmed a multifocal tall cell variant PTC together with a 12 mm minimally invasive FTC in the ipsilateral lobe. While the central compartment demonstrated metastatic PTC, the lateral compartment contained PTC metastases alongside a 15 mm large follicular-patterned mass in a separate lymph node. As the cells lacked PTC associated nuclear changes, the possibility of a lateral lymph node metastasis of FTC was considered, with the possibility of ectopic thyroid tissue as a differential diagnosis. By utilizing next-generation sequencing, a Q61R NRAS mutation was pinpointed, thus proving the tissue as tumorous. The patient underwent radioiodine treatment and is currently monitored following a negative whole-body scan.</p><p><strong>Conclusions: </strong>This is probably the first case report of a patient with co-existing lateral lymph node PTC and FTC metastases. Consulting previous publications, there is currently a gap of knowledge in terms of how patients with regional FTC metastases should be followed-up and treated, especially when co-occurring with spread high-risk PTC subtypes. Moreover, what guides a seemingly indolent FTC to spread via the lymphatic system remains to be defined from a molecular standpoint.</p>","PeriodicalId":39048,"journal":{"name":"Thyroid Research","volume":null,"pages":null},"PeriodicalIF":1.9000,"publicationDate":"2022-02-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8815265/pdf/","citationCount":"5","resultStr":"{\"title\":\"Synchronous lateral lymph node metastases from papillary and follicular thyroid carcinoma: case report and review of the literature.\",\"authors\":\"Adam Stenman, Magnus Kjellman, Jan Zedenius, C Christofer Juhlin\",\"doi\":\"10.1186/s13044-022-00120-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Follicular thyroid carcinomas (FTCs) rarely metastasize to regional lymph nodes, and descriptions of synchronous lateral lymph node metastases of FTC and papillary thyroid carcinoma (PTC) are lacking.</p><p><strong>Case presentation: </strong>We describe a 43-year-old female with a preoperative cytology indicating a right-sided PTC with lateral lymph node metastases. She underwent a total thyroidectomy and central and lateral lymph node dissection, and histopathology confirmed a multifocal tall cell variant PTC together with a 12 mm minimally invasive FTC in the ipsilateral lobe. While the central compartment demonstrated metastatic PTC, the lateral compartment contained PTC metastases alongside a 15 mm large follicular-patterned mass in a separate lymph node. As the cells lacked PTC associated nuclear changes, the possibility of a lateral lymph node metastasis of FTC was considered, with the possibility of ectopic thyroid tissue as a differential diagnosis. By utilizing next-generation sequencing, a Q61R NRAS mutation was pinpointed, thus proving the tissue as tumorous. The patient underwent radioiodine treatment and is currently monitored following a negative whole-body scan.</p><p><strong>Conclusions: </strong>This is probably the first case report of a patient with co-existing lateral lymph node PTC and FTC metastases. Consulting previous publications, there is currently a gap of knowledge in terms of how patients with regional FTC metastases should be followed-up and treated, especially when co-occurring with spread high-risk PTC subtypes. Moreover, what guides a seemingly indolent FTC to spread via the lymphatic system remains to be defined from a molecular standpoint.</p>\",\"PeriodicalId\":39048,\"journal\":{\"name\":\"Thyroid Research\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2022-02-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8815265/pdf/\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Thyroid Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13044-022-00120-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-022-00120-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Synchronous lateral lymph node metastases from papillary and follicular thyroid carcinoma: case report and review of the literature.
Background: Follicular thyroid carcinomas (FTCs) rarely metastasize to regional lymph nodes, and descriptions of synchronous lateral lymph node metastases of FTC and papillary thyroid carcinoma (PTC) are lacking.
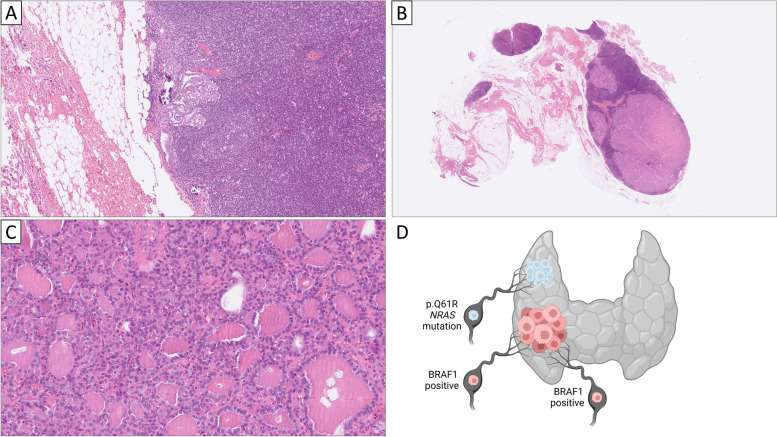
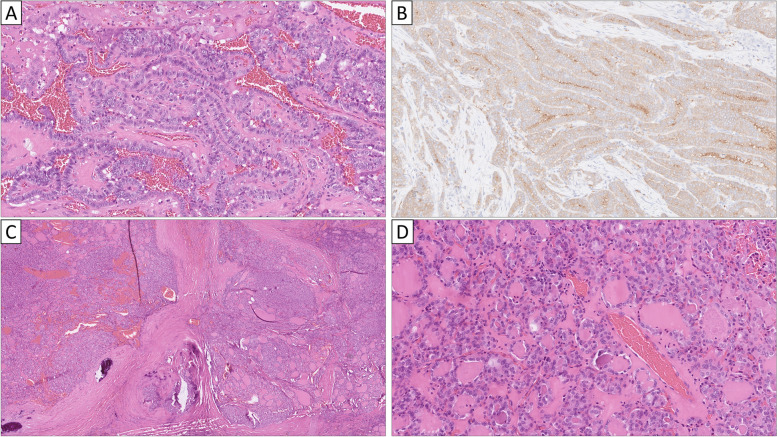
Case presentation: We describe a 43-year-old female with a preoperative cytology indicating a right-sided PTC with lateral lymph node metastases. She underwent a total thyroidectomy and central and lateral lymph node dissection, and histopathology confirmed a multifocal tall cell variant PTC together with a 12 mm minimally invasive FTC in the ipsilateral lobe. While the central compartment demonstrated metastatic PTC, the lateral compartment contained PTC metastases alongside a 15 mm large follicular-patterned mass in a separate lymph node. As the cells lacked PTC associated nuclear changes, the possibility of a lateral lymph node metastasis of FTC was considered, with the possibility of ectopic thyroid tissue as a differential diagnosis. By utilizing next-generation sequencing, a Q61R NRAS mutation was pinpointed, thus proving the tissue as tumorous. The patient underwent radioiodine treatment and is currently monitored following a negative whole-body scan.
Conclusions: This is probably the first case report of a patient with co-existing lateral lymph node PTC and FTC metastases. Consulting previous publications, there is currently a gap of knowledge in terms of how patients with regional FTC metastases should be followed-up and treated, especially when co-occurring with spread high-risk PTC subtypes. Moreover, what guides a seemingly indolent FTC to spread via the lymphatic system remains to be defined from a molecular standpoint.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
