{"title":"应用凝血-纤溶标志物预测Stanford A型急性主动脉夹层。","authors":"Daisuke Arima, Yoshihiro Suematsu, Kanan Kurahashi, Satoshi Nishi, Akihiro Yoshimoto","doi":"10.1177/20480040211047122","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Coagulation-fibrinolysis markers are widely used for the diagnosis of Stanford type A acute aortic dissection (SAAAD). However, the role of these markers in estimating prognosis remains unclear.</p><p><strong>Methods: </strong>A single-center retrospective study was conducted to identify the relationship between preoperative D-dimer and fibrinogen levels on SAAAD postoperative early prognosis.</p><p><strong>Results: </strong>Of 238 SAAAD patients who underwent surgery between January 2012 and December 2018, 201 (84.5%) and 37 (15.5%) patients constituted the survival and non-survival groups, respectively, 30 days after surgery. D-dimer and fibrinogen levels in the survival and non-survival groups were 45.2 ± 74.3 vs. 91.5 ± 103.6 μg/mL (<i>p</i> = 0.014) and 224.3 ± 95.6 vs. 179.9 ± 96.7 μg/mL (<i>p</i> = 0.012), respectively. According to logistic predictor analysis of 30-day mortality, significant factors showed patent type (OR 10.89, 95% CI 1.66-20.31) and malperfusion (OR 4.63, 95% CI 1.74-12.32). Increasing D-dimer (per +10 μg/mL) and decreasing fibrinogen (per -10 μg/mL) were significantly associated with patent type and malperfusion. Receiver operating characteristic analysis was performed to distinguish between survival and non-survival. The cutoff value of D-dimer was 60 μg/mL (sensitivity 61.1%; specificity 82.5%; area under curve [AUC] 0.713 ± 0.083); fibrinogen was 150 mg/dL (sensitivity 44.4%; specificity 84.0%; AUC 0.647 ± 0.092). Kaplan-Meier survival curve analysis showed that patients with D-dimer levels > 60 μg/mL and fibrinogen levels < 150 mg/dL had significantly low survival rates at 30 days after surgery (60.0%, <i>p</i> < 0.001).</p><p><strong>Conclusion: </strong>Preoperative coagulation-fibrinolysis markers may be useful for predicting early prognosis in SAAAD.</p>","PeriodicalId":30457,"journal":{"name":"JRSM Cardiovascular Disease","volume":"10 ","pages":"20480040211047122"},"PeriodicalIF":1.5000,"publicationDate":"2021-11-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/59/09/10.1177_20480040211047122.PMC8613881.pdf","citationCount":"2","resultStr":"{\"title\":\"Use of coagulation-fibrinolysis markers for prognostication of Stanford type A acute aortic dissection.\",\"authors\":\"Daisuke Arima, Yoshihiro Suematsu, Kanan Kurahashi, Satoshi Nishi, Akihiro Yoshimoto\",\"doi\":\"10.1177/20480040211047122\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Coagulation-fibrinolysis markers are widely used for the diagnosis of Stanford type A acute aortic dissection (SAAAD). However, the role of these markers in estimating prognosis remains unclear.</p><p><strong>Methods: </strong>A single-center retrospective study was conducted to identify the relationship between preoperative D-dimer and fibrinogen levels on SAAAD postoperative early prognosis.</p><p><strong>Results: </strong>Of 238 SAAAD patients who underwent surgery between January 2012 and December 2018, 201 (84.5%) and 37 (15.5%) patients constituted the survival and non-survival groups, respectively, 30 days after surgery. D-dimer and fibrinogen levels in the survival and non-survival groups were 45.2 ± 74.3 vs. 91.5 ± 103.6 μg/mL (<i>p</i> = 0.014) and 224.3 ± 95.6 vs. 179.9 ± 96.7 μg/mL (<i>p</i> = 0.012), respectively. According to logistic predictor analysis of 30-day mortality, significant factors showed patent type (OR 10.89, 95% CI 1.66-20.31) and malperfusion (OR 4.63, 95% CI 1.74-12.32). Increasing D-dimer (per +10 μg/mL) and decreasing fibrinogen (per -10 μg/mL) were significantly associated with patent type and malperfusion. Receiver operating characteristic analysis was performed to distinguish between survival and non-survival. The cutoff value of D-dimer was 60 μg/mL (sensitivity 61.1%; specificity 82.5%; area under curve [AUC] 0.713 ± 0.083); fibrinogen was 150 mg/dL (sensitivity 44.4%; specificity 84.0%; AUC 0.647 ± 0.092). Kaplan-Meier survival curve analysis showed that patients with D-dimer levels > 60 μg/mL and fibrinogen levels < 150 mg/dL had significantly low survival rates at 30 days after surgery (60.0%, <i>p</i> < 0.001).</p><p><strong>Conclusion: </strong>Preoperative coagulation-fibrinolysis markers may be useful for predicting early prognosis in SAAAD.</p>\",\"PeriodicalId\":30457,\"journal\":{\"name\":\"JRSM Cardiovascular Disease\",\"volume\":\"10 \",\"pages\":\"20480040211047122\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2021-11-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/59/09/10.1177_20480040211047122.PMC8613881.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JRSM Cardiovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20480040211047122\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20480040211047122","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Use of coagulation-fibrinolysis markers for prognostication of Stanford type A acute aortic dissection.
Purpose: Coagulation-fibrinolysis markers are widely used for the diagnosis of Stanford type A acute aortic dissection (SAAAD). However, the role of these markers in estimating prognosis remains unclear.
Methods: A single-center retrospective study was conducted to identify the relationship between preoperative D-dimer and fibrinogen levels on SAAAD postoperative early prognosis.
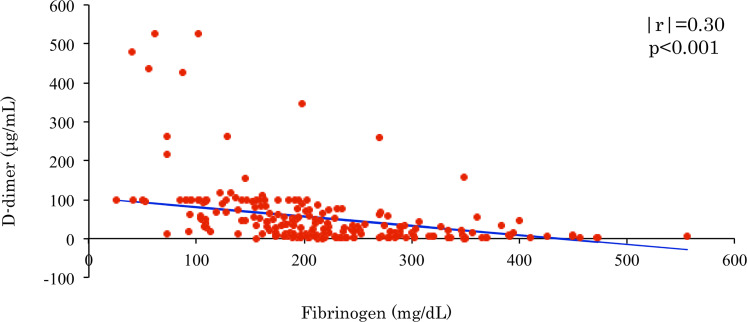
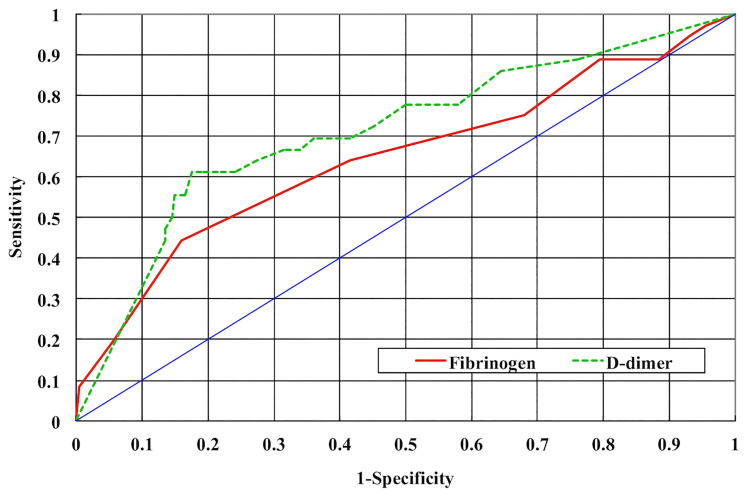
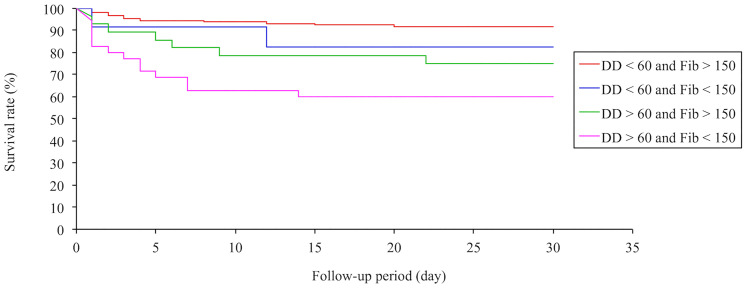
Results: Of 238 SAAAD patients who underwent surgery between January 2012 and December 2018, 201 (84.5%) and 37 (15.5%) patients constituted the survival and non-survival groups, respectively, 30 days after surgery. D-dimer and fibrinogen levels in the survival and non-survival groups were 45.2 ± 74.3 vs. 91.5 ± 103.6 μg/mL (p = 0.014) and 224.3 ± 95.6 vs. 179.9 ± 96.7 μg/mL (p = 0.012), respectively. According to logistic predictor analysis of 30-day mortality, significant factors showed patent type (OR 10.89, 95% CI 1.66-20.31) and malperfusion (OR 4.63, 95% CI 1.74-12.32). Increasing D-dimer (per +10 μg/mL) and decreasing fibrinogen (per -10 μg/mL) were significantly associated with patent type and malperfusion. Receiver operating characteristic analysis was performed to distinguish between survival and non-survival. The cutoff value of D-dimer was 60 μg/mL (sensitivity 61.1%; specificity 82.5%; area under curve [AUC] 0.713 ± 0.083); fibrinogen was 150 mg/dL (sensitivity 44.4%; specificity 84.0%; AUC 0.647 ± 0.092). Kaplan-Meier survival curve analysis showed that patients with D-dimer levels > 60 μg/mL and fibrinogen levels < 150 mg/dL had significantly low survival rates at 30 days after surgery (60.0%, p < 0.001).
Conclusion: Preoperative coagulation-fibrinolysis markers may be useful for predicting early prognosis in SAAAD.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
