Serhiy Semenov, Mohd Syafiq Ismail, Fintan O'Hara, Sandeep Sihag, Barbara Ryan, Anthony O'Connor, Sarah O'Donnell, Deirdre McNamara
{"title":"添加蓖麻油作为结肠胶囊方案的助推器,显著提高完成率和息肉检出率。","authors":"Serhiy Semenov, Mohd Syafiq Ismail, Fintan O'Hara, Sandeep Sihag, Barbara Ryan, Anthony O'Connor, Sarah O'Donnell, Deirdre McNamara","doi":"10.4292/wjgpt.v12.i6.103","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Incomplete excretion rates are problematic for colon capsule endoscopy (CCE). Widely available booster regimens are suboptimal. Recently published data on one day preparation CCE protocol using castor oil appeared effective.</p><p><strong>Aim: </strong>To assess the impact of adding castor oil to a standard split-dose (2-d) preparation in an unselected Western patient cohort.</p><p><strong>Methods: </strong>All patients aged 18 or more referred to our unit for a CCE over a 5-mo period were prospectively recruited. Controls were retrospectively identified from our CCE database. All patients received split bowel preparation with Moviprep<sup>®</sup> [polyethylene glycol (PEG)-3350, sodium sulphate, sodium chloride, potassium chloride, sodium ascorbate and ascorbic acid for oral solution; Norgine B. V, United States], a PEG-based solution used predominantly in our colonoscopy practice. Control booster regimen included Moviprep<sup>®</sup> with 750 mL of water (booster 1) on reaching the small bowel. A further dose of Moviprep<sup>®</sup> with 250 mL of water was given 3 h later and a bisacodyl suppository (Dulcolax<sup>®</sup>) 10 mg after 8 h, if the capsule was not excreted. In addition to our standard booster regimen, cases received an additional 15 mL of castor oil given at the time of booster 1. A nested case control design with 2:1 ratio (control:case) was employed. Basic demographics, completion rates, image quality, colonic transit time, diagnostic yield and polyp detection were compared between groups, using a student <i>t</i> or chi-square tests as appropriate.</p><p><strong>Results: </strong>One hundred and eighty-six CCEs [mean age 60 years (18-97), 56% females, <i>n</i> = 104], including 62 cases have been analysed. Indication breakdown included 96 polyp surveillance (51.6%), 42 lower gastrointestinal symptoms (22.6%), 28 due to incomplete colonoscopy (15%), 18 anaemia (9.7%) and 2 inflammatory bowel disease surveillance (1.1%). Overall, CCE completion was 77% (144/186), image quality was adequate/diagnostic in 91% (170/186), mean colonic transit time was 3.5 h (0.25-13), and the polyp detection rate was 57% (106/186). Completion rates were significantly higher with castor oil, 87% cases (54/62) <i>vs</i> 73% controls (90/124), <i>P</i> = 0.01. The number needed to treat with castor oil to result in an additional complete CCE study was 7, absolute risk reduction = 14.52%, 95% confidence interval (CI): 3.06- 25.97. This effect of castor oil on excretion rates was more significant in the over 60 s, <i>P</i> < 0.03, and in females, <i>P</i> < 0.025. Similarly, polyp detection rates were higher in cases 82% (51/62) <i>vs</i> controls 44% (55/124), <i>P</i> = 0.0001, odds ratio 5.8, 95%CI: 2.77-12.21. Colonic transit times were similar, 3.2 h and 3.8 h, respectively. Image quality was similar, reported as adequate/diagnostic in 90% (56/62) <i>vs</i> 92% (114/124).</p><p><strong>Conclusion: </strong>In our capsule endoscopy centre, castor oil addition as a CCE booster significantly improved completion rates and polyp detection in an unselected Western cohort.</p>","PeriodicalId":23755,"journal":{"name":"World Journal of Gastrointestinal Pharmacology and Therapeutics","volume":"12 6","pages":"103-112"},"PeriodicalIF":0.0000,"publicationDate":"2021-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/57/4b/WJGPT-12-103.PMC8611183.pdf","citationCount":"7","resultStr":"{\"title\":\"Addition of castor oil as a booster in colon capsule regimens significantly improves completion rates and polyp detection.\",\"authors\":\"Serhiy Semenov, Mohd Syafiq Ismail, Fintan O'Hara, Sandeep Sihag, Barbara Ryan, Anthony O'Connor, Sarah O'Donnell, Deirdre McNamara\",\"doi\":\"10.4292/wjgpt.v12.i6.103\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Incomplete excretion rates are problematic for colon capsule endoscopy (CCE). Widely available booster regimens are suboptimal. Recently published data on one day preparation CCE protocol using castor oil appeared effective.</p><p><strong>Aim: </strong>To assess the impact of adding castor oil to a standard split-dose (2-d) preparation in an unselected Western patient cohort.</p><p><strong>Methods: </strong>All patients aged 18 or more referred to our unit for a CCE over a 5-mo period were prospectively recruited. Controls were retrospectively identified from our CCE database. All patients received split bowel preparation with Moviprep<sup>®</sup> [polyethylene glycol (PEG)-3350, sodium sulphate, sodium chloride, potassium chloride, sodium ascorbate and ascorbic acid for oral solution; Norgine B. V, United States], a PEG-based solution used predominantly in our colonoscopy practice. Control booster regimen included Moviprep<sup>®</sup> with 750 mL of water (booster 1) on reaching the small bowel. A further dose of Moviprep<sup>®</sup> with 250 mL of water was given 3 h later and a bisacodyl suppository (Dulcolax<sup>®</sup>) 10 mg after 8 h, if the capsule was not excreted. In addition to our standard booster regimen, cases received an additional 15 mL of castor oil given at the time of booster 1. A nested case control design with 2:1 ratio (control:case) was employed. Basic demographics, completion rates, image quality, colonic transit time, diagnostic yield and polyp detection were compared between groups, using a student <i>t</i> or chi-square tests as appropriate.</p><p><strong>Results: </strong>One hundred and eighty-six CCEs [mean age 60 years (18-97), 56% females, <i>n</i> = 104], including 62 cases have been analysed. Indication breakdown included 96 polyp surveillance (51.6%), 42 lower gastrointestinal symptoms (22.6%), 28 due to incomplete colonoscopy (15%), 18 anaemia (9.7%) and 2 inflammatory bowel disease surveillance (1.1%). Overall, CCE completion was 77% (144/186), image quality was adequate/diagnostic in 91% (170/186), mean colonic transit time was 3.5 h (0.25-13), and the polyp detection rate was 57% (106/186). Completion rates were significantly higher with castor oil, 87% cases (54/62) <i>vs</i> 73% controls (90/124), <i>P</i> = 0.01. The number needed to treat with castor oil to result in an additional complete CCE study was 7, absolute risk reduction = 14.52%, 95% confidence interval (CI): 3.06- 25.97. This effect of castor oil on excretion rates was more significant in the over 60 s, <i>P</i> < 0.03, and in females, <i>P</i> < 0.025. Similarly, polyp detection rates were higher in cases 82% (51/62) <i>vs</i> controls 44% (55/124), <i>P</i> = 0.0001, odds ratio 5.8, 95%CI: 2.77-12.21. Colonic transit times were similar, 3.2 h and 3.8 h, respectively. Image quality was similar, reported as adequate/diagnostic in 90% (56/62) <i>vs</i> 92% (114/124).</p><p><strong>Conclusion: </strong>In our capsule endoscopy centre, castor oil addition as a CCE booster significantly improved completion rates and polyp detection in an unselected Western cohort.</p>\",\"PeriodicalId\":23755,\"journal\":{\"name\":\"World Journal of Gastrointestinal Pharmacology and Therapeutics\",\"volume\":\"12 6\",\"pages\":\"103-112\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-11-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/57/4b/WJGPT-12-103.PMC8611183.pdf\",\"citationCount\":\"7\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Pharmacology and Therapeutics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4292/wjgpt.v12.i6.103\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Pharmacology and Therapeutics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4292/wjgpt.v12.i6.103","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Addition of castor oil as a booster in colon capsule regimens significantly improves completion rates and polyp detection.
Background: Incomplete excretion rates are problematic for colon capsule endoscopy (CCE). Widely available booster regimens are suboptimal. Recently published data on one day preparation CCE protocol using castor oil appeared effective.
Aim: To assess the impact of adding castor oil to a standard split-dose (2-d) preparation in an unselected Western patient cohort.
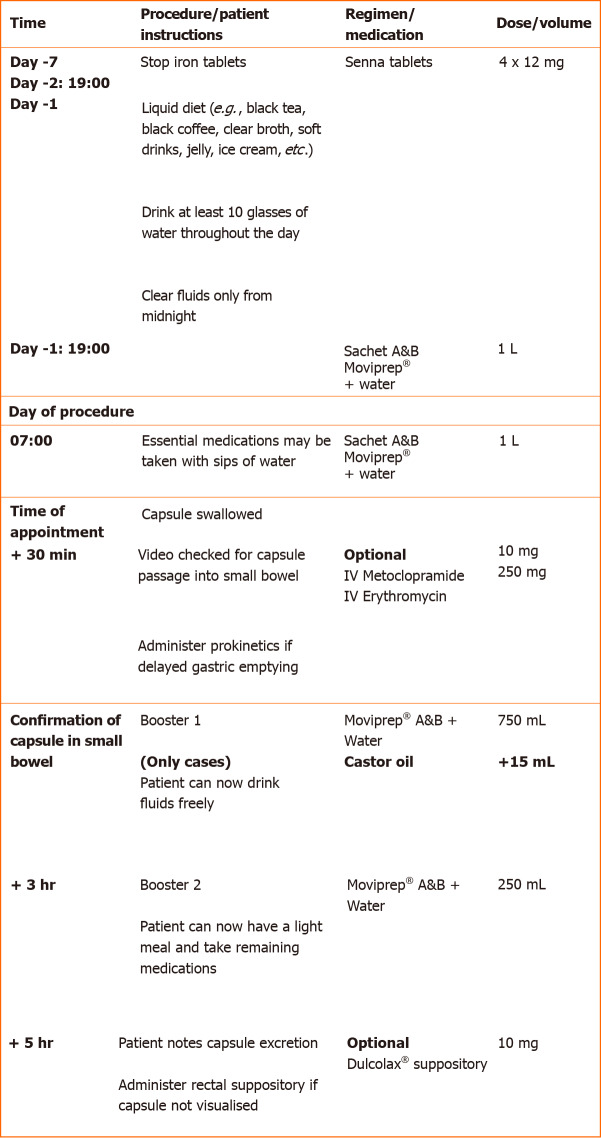
Methods: All patients aged 18 or more referred to our unit for a CCE over a 5-mo period were prospectively recruited. Controls were retrospectively identified from our CCE database. All patients received split bowel preparation with Moviprep® [polyethylene glycol (PEG)-3350, sodium sulphate, sodium chloride, potassium chloride, sodium ascorbate and ascorbic acid for oral solution; Norgine B. V, United States], a PEG-based solution used predominantly in our colonoscopy practice. Control booster regimen included Moviprep® with 750 mL of water (booster 1) on reaching the small bowel. A further dose of Moviprep® with 250 mL of water was given 3 h later and a bisacodyl suppository (Dulcolax®) 10 mg after 8 h, if the capsule was not excreted. In addition to our standard booster regimen, cases received an additional 15 mL of castor oil given at the time of booster 1. A nested case control design with 2:1 ratio (control:case) was employed. Basic demographics, completion rates, image quality, colonic transit time, diagnostic yield and polyp detection were compared between groups, using a student t or chi-square tests as appropriate.
Results: One hundred and eighty-six CCEs [mean age 60 years (18-97), 56% females, n = 104], including 62 cases have been analysed. Indication breakdown included 96 polyp surveillance (51.6%), 42 lower gastrointestinal symptoms (22.6%), 28 due to incomplete colonoscopy (15%), 18 anaemia (9.7%) and 2 inflammatory bowel disease surveillance (1.1%). Overall, CCE completion was 77% (144/186), image quality was adequate/diagnostic in 91% (170/186), mean colonic transit time was 3.5 h (0.25-13), and the polyp detection rate was 57% (106/186). Completion rates were significantly higher with castor oil, 87% cases (54/62) vs 73% controls (90/124), P = 0.01. The number needed to treat with castor oil to result in an additional complete CCE study was 7, absolute risk reduction = 14.52%, 95% confidence interval (CI): 3.06- 25.97. This effect of castor oil on excretion rates was more significant in the over 60 s, P < 0.03, and in females, P < 0.025. Similarly, polyp detection rates were higher in cases 82% (51/62) vs controls 44% (55/124), P = 0.0001, odds ratio 5.8, 95%CI: 2.77-12.21. Colonic transit times were similar, 3.2 h and 3.8 h, respectively. Image quality was similar, reported as adequate/diagnostic in 90% (56/62) vs 92% (114/124).
Conclusion: In our capsule endoscopy centre, castor oil addition as a CCE booster significantly improved completion rates and polyp detection in an unselected Western cohort.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
