{"title":"COVID-19和子痫前期:妊娠的重叠特征","authors":"Ramasamy Sathiya, Jayanthi Rajendran, Saravanan Sumathi","doi":"10.5041/RMMJ.10464","DOIUrl":null,"url":null,"abstract":"<p><p>Coronavirus disease 2019 (COVID-19) is a global respiratory disease with unique features that have placed all medical professionals in an alarming situation. Preeclampsia is a hypertensive disorder of pregnancy affecting 8%-10% of India's pregnant population. Assuming that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) enters host cells through the angiotensin-converting enzyme 2 (ACE2) receptor, the resulting symptoms are due to vasoconstriction, caused by disturbances in the renin-angiotensin system (RAS). Other features of preeclampsia include endothelial dysfunction due to placental ischemia, leading to imbalances in angiogenic and antiangiogenic factors which result in increased blood pressure, proteinuria, altered hepatic enzymes, renal failure, and thrombocytopenia, amongst others. The increased prevalence of preeclampsia that was seen among mothers with SARS-CoV-2 infection might be due to misdiagnosis, as COVID-19 and preeclampsia have coincidental medical features. The major similarities of SARS-CoV-2-infected and preeclamptic women are a rise in pro-inflammatory cytokines, and increased serum ferritin and thrombocytopenia. Therefore, differential diagnosis might be difficult in pregnant women with COVID-19 who present with hypertension and proteinuria, thrombocytopenia, or elevated liver enzymes. The most promising markers for earlier diagnosis of preeclampsia is soluble endoglin (sEng), pregnancy-associated plasma protein-A (PAPP-A), soluble fms-like tyrosine kinase 1 (sFlt-1), and placental growth factor (PlGF). Due to placental hypoxia, sFlt-1 will be overproduced, thus inhibiting PlGF, and this alteration will be observed in the circulation five weeks or more before the onset of symptoms. The sFlt-1/PlGF ratio may also be modified via infectious states, but unregulated levels of those mediators are related to placental insufficiency. Hence, pregnant women with COVID-19 may develop a preeclampsia-like syndrome that might be differentiated properly by angiogenic markers to avoid unnecessary interventions and induced preterm labor.</p>","PeriodicalId":46408,"journal":{"name":"Rambam Maimonides Medical Journal","volume":"13 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2022-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8798587/pdf/","citationCount":"18","resultStr":"{\"title\":\"COVID-19 and Preeclampsia: Overlapping Features in Pregnancy.\",\"authors\":\"Ramasamy Sathiya, Jayanthi Rajendran, Saravanan Sumathi\",\"doi\":\"10.5041/RMMJ.10464\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Coronavirus disease 2019 (COVID-19) is a global respiratory disease with unique features that have placed all medical professionals in an alarming situation. Preeclampsia is a hypertensive disorder of pregnancy affecting 8%-10% of India's pregnant population. Assuming that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) enters host cells through the angiotensin-converting enzyme 2 (ACE2) receptor, the resulting symptoms are due to vasoconstriction, caused by disturbances in the renin-angiotensin system (RAS). Other features of preeclampsia include endothelial dysfunction due to placental ischemia, leading to imbalances in angiogenic and antiangiogenic factors which result in increased blood pressure, proteinuria, altered hepatic enzymes, renal failure, and thrombocytopenia, amongst others. The increased prevalence of preeclampsia that was seen among mothers with SARS-CoV-2 infection might be due to misdiagnosis, as COVID-19 and preeclampsia have coincidental medical features. The major similarities of SARS-CoV-2-infected and preeclamptic women are a rise in pro-inflammatory cytokines, and increased serum ferritin and thrombocytopenia. Therefore, differential diagnosis might be difficult in pregnant women with COVID-19 who present with hypertension and proteinuria, thrombocytopenia, or elevated liver enzymes. The most promising markers for earlier diagnosis of preeclampsia is soluble endoglin (sEng), pregnancy-associated plasma protein-A (PAPP-A), soluble fms-like tyrosine kinase 1 (sFlt-1), and placental growth factor (PlGF). Due to placental hypoxia, sFlt-1 will be overproduced, thus inhibiting PlGF, and this alteration will be observed in the circulation five weeks or more before the onset of symptoms. The sFlt-1/PlGF ratio may also be modified via infectious states, but unregulated levels of those mediators are related to placental insufficiency. Hence, pregnant women with COVID-19 may develop a preeclampsia-like syndrome that might be differentiated properly by angiogenic markers to avoid unnecessary interventions and induced preterm labor.</p>\",\"PeriodicalId\":46408,\"journal\":{\"name\":\"Rambam Maimonides Medical Journal\",\"volume\":\"13 1\",\"pages\":\"\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-01-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8798587/pdf/\",\"citationCount\":\"18\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rambam Maimonides Medical Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5041/RMMJ.10464\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rambam Maimonides Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5041/RMMJ.10464","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
COVID-19 and Preeclampsia: Overlapping Features in Pregnancy.
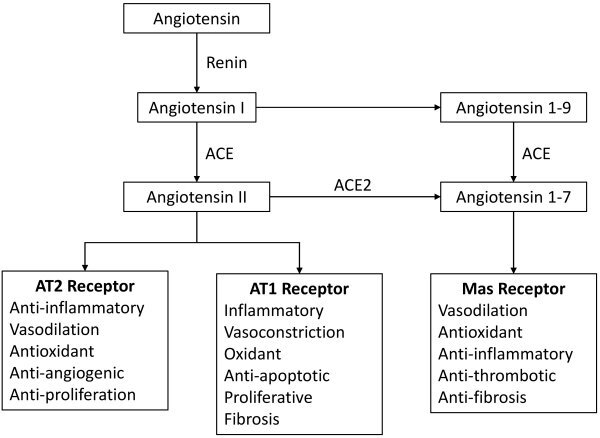
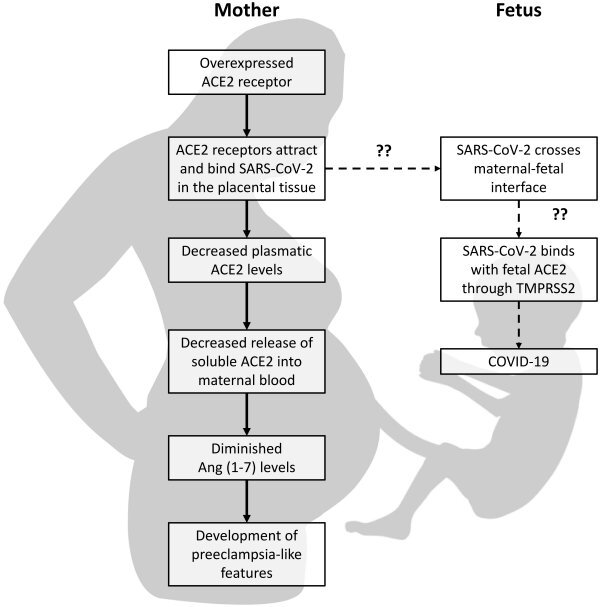
Coronavirus disease 2019 (COVID-19) is a global respiratory disease with unique features that have placed all medical professionals in an alarming situation. Preeclampsia is a hypertensive disorder of pregnancy affecting 8%-10% of India's pregnant population. Assuming that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) enters host cells through the angiotensin-converting enzyme 2 (ACE2) receptor, the resulting symptoms are due to vasoconstriction, caused by disturbances in the renin-angiotensin system (RAS). Other features of preeclampsia include endothelial dysfunction due to placental ischemia, leading to imbalances in angiogenic and antiangiogenic factors which result in increased blood pressure, proteinuria, altered hepatic enzymes, renal failure, and thrombocytopenia, amongst others. The increased prevalence of preeclampsia that was seen among mothers with SARS-CoV-2 infection might be due to misdiagnosis, as COVID-19 and preeclampsia have coincidental medical features. The major similarities of SARS-CoV-2-infected and preeclamptic women are a rise in pro-inflammatory cytokines, and increased serum ferritin and thrombocytopenia. Therefore, differential diagnosis might be difficult in pregnant women with COVID-19 who present with hypertension and proteinuria, thrombocytopenia, or elevated liver enzymes. The most promising markers for earlier diagnosis of preeclampsia is soluble endoglin (sEng), pregnancy-associated plasma protein-A (PAPP-A), soluble fms-like tyrosine kinase 1 (sFlt-1), and placental growth factor (PlGF). Due to placental hypoxia, sFlt-1 will be overproduced, thus inhibiting PlGF, and this alteration will be observed in the circulation five weeks or more before the onset of symptoms. The sFlt-1/PlGF ratio may also be modified via infectious states, but unregulated levels of those mediators are related to placental insufficiency. Hence, pregnant women with COVID-19 may develop a preeclampsia-like syndrome that might be differentiated properly by angiogenic markers to avoid unnecessary interventions and induced preterm labor.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
