Sean C Dougherty, Nisa Desai, Helen P Cathro, Amanda Renaghan
{"title":"继发于伊匹单抗的 IgA 肾病。","authors":"Sean C Dougherty, Nisa Desai, Helen P Cathro, Amanda Renaghan","doi":"10.1159/000519169","DOIUrl":null,"url":null,"abstract":"<p><p>Ipilimumab is a human monoclonal antibody targeting cytotoxic T-lymphocyte-associated protein 4 approved for the treatment of non-small-cell lung cancer (NSCLC) and other malignancies. Despite a high prevalence of other immune-related adverse events (irAEs), checkpoint inhibitor (CPI)-related nephrotoxicity has been reported less frequently. In this clinical case report, we describe the evaluation of a 70-year-old female with stage IV NSCLC who presented with nephrotic range proteinuria 4 weeks after receiving her first cycle of ipilimumab. She underwent a renal biopsy and was found to have IgA nephropathy that was presumed to be secondary to ipilimumab use, given recent initiation of therapy and clinical history. Unfortunately, despite prompt initiation of corticosteroids, her acute kidney injury progressed and she required hemodialysis, later transitioning to hospice. To our knowledge, this is one of few reported cases of IgA nephropathy secondary to CPI use. With increasing use of CPIs, this case further emphasizes the need for continued surveillance for irAEs, which can occur at any point in a patient's treatment course.</p>","PeriodicalId":9599,"journal":{"name":"Case Reports in Nephrology and Dialysis","volume":"11 3","pages":"327-333"},"PeriodicalIF":0.9000,"publicationDate":"2021-11-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a1/52/cnd-0011-0327.PMC8647129.pdf","citationCount":"0","resultStr":"{\"title\":\"IgA Nephropathy Secondary to Ipilimumab Use.\",\"authors\":\"Sean C Dougherty, Nisa Desai, Helen P Cathro, Amanda Renaghan\",\"doi\":\"10.1159/000519169\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Ipilimumab is a human monoclonal antibody targeting cytotoxic T-lymphocyte-associated protein 4 approved for the treatment of non-small-cell lung cancer (NSCLC) and other malignancies. Despite a high prevalence of other immune-related adverse events (irAEs), checkpoint inhibitor (CPI)-related nephrotoxicity has been reported less frequently. In this clinical case report, we describe the evaluation of a 70-year-old female with stage IV NSCLC who presented with nephrotic range proteinuria 4 weeks after receiving her first cycle of ipilimumab. She underwent a renal biopsy and was found to have IgA nephropathy that was presumed to be secondary to ipilimumab use, given recent initiation of therapy and clinical history. Unfortunately, despite prompt initiation of corticosteroids, her acute kidney injury progressed and she required hemodialysis, later transitioning to hospice. To our knowledge, this is one of few reported cases of IgA nephropathy secondary to CPI use. With increasing use of CPIs, this case further emphasizes the need for continued surveillance for irAEs, which can occur at any point in a patient's treatment course.</p>\",\"PeriodicalId\":9599,\"journal\":{\"name\":\"Case Reports in Nephrology and Dialysis\",\"volume\":\"11 3\",\"pages\":\"327-333\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2021-11-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a1/52/cnd-0011-0327.PMC8647129.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Nephrology and Dialysis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000519169\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology and Dialysis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000519169","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
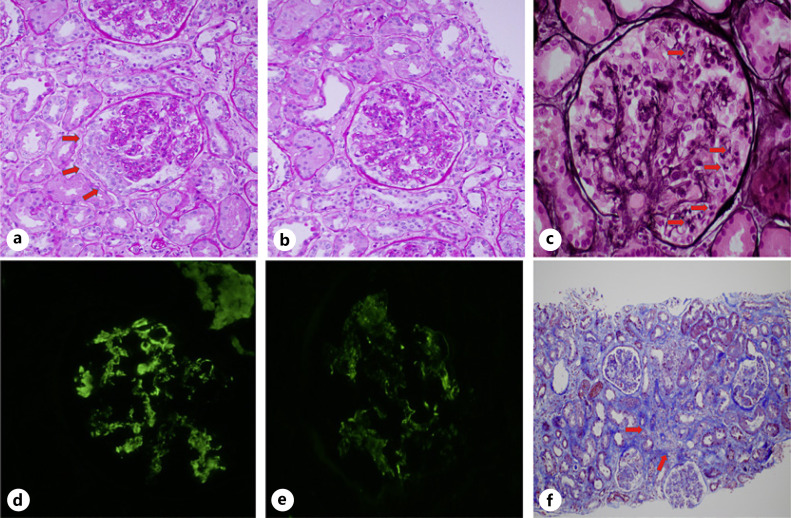
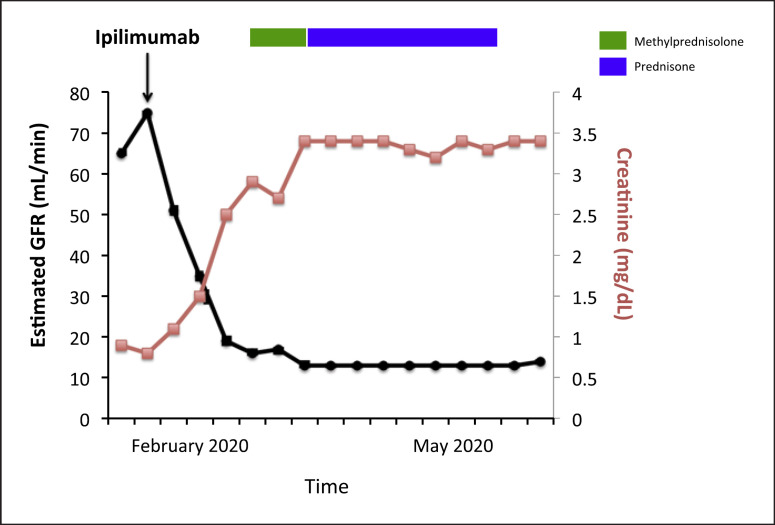
伊匹单抗是一种靶向细胞毒性T淋巴细胞相关蛋白4的人类单克隆抗体,已被批准用于治疗非小细胞肺癌(NSCLC)和其他恶性肿瘤。尽管其他免疫相关不良事件(irAEs)的发生率很高,但与检查点抑制剂(CPI)相关的肾毒性却鲜有报道。在这份临床病例报告中,我们描述了对一名患有 IV 期 NSCLC 的 70 岁女性患者的评估,她在接受第一个周期的伊匹单抗治疗 4 周后出现肾病范围蛋白尿。她接受了肾活检,发现患有IgA肾病,考虑到最近开始的治疗和临床病史,推测该病是继发于伊匹单抗的使用。不幸的是,尽管及时使用了皮质类固醇,她的急性肾损伤仍在发展,需要进行血液透析,后来转入临终关怀。据我们所知,这是极少数因使用 CPI 而继发 IgA 肾病的病例之一。随着 CPI 的使用越来越多,本病例进一步强调了持续监测虹膜急性肾损伤的必要性,虹膜急性肾损伤可能发生在患者治疗过程的任何阶段。
Ipilimumab is a human monoclonal antibody targeting cytotoxic T-lymphocyte-associated protein 4 approved for the treatment of non-small-cell lung cancer (NSCLC) and other malignancies. Despite a high prevalence of other immune-related adverse events (irAEs), checkpoint inhibitor (CPI)-related nephrotoxicity has been reported less frequently. In this clinical case report, we describe the evaluation of a 70-year-old female with stage IV NSCLC who presented with nephrotic range proteinuria 4 weeks after receiving her first cycle of ipilimumab. She underwent a renal biopsy and was found to have IgA nephropathy that was presumed to be secondary to ipilimumab use, given recent initiation of therapy and clinical history. Unfortunately, despite prompt initiation of corticosteroids, her acute kidney injury progressed and she required hemodialysis, later transitioning to hospice. To our knowledge, this is one of few reported cases of IgA nephropathy secondary to CPI use. With increasing use of CPIs, this case further emphasizes the need for continued surveillance for irAEs, which can occur at any point in a patient's treatment course.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of nephrology and dialysis, including genetic susceptibility, clinical presentation, diagnosis, treatment or prevention, toxicities of therapy, critical care, supportive care, quality-of-life and survival issues. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
