Januario E Castro, Paula A Lengerke-Diaz, Juliana Velez Lujan, Michael Y Choi, Eider F Moreno-Cortes, Jose V Forero, Juan Esteban Garcia-Robledo, Chaja Jacobs, Colin McCarthy, Alaina Heinen, Carlos I Amaya-Chanaga, Thomas J Kipps
{"title":"一项单臂、开放标签、1b/2期临床试验NCT0231576: Ibrutinib + Obinutuzumab作为慢性淋巴细胞白血病的一线治疗与较低的输注相关反应率和Ibrutinib停药后持续缓解相关","authors":"Januario E Castro, Paula A Lengerke-Diaz, Juliana Velez Lujan, Michael Y Choi, Eider F Moreno-Cortes, Jose V Forero, Juan Esteban Garcia-Robledo, Chaja Jacobs, Colin McCarthy, Alaina Heinen, Carlos I Amaya-Chanaga, Thomas J Kipps","doi":"10.1155/2022/4450824","DOIUrl":null,"url":null,"abstract":"<p><p>Ibrutinib-based therapies are costly and require continuous administration. We hypothesized combining BTK inhibition with anti-CD20 monoclonal antibodies would yield deep remissions allowing discontinuation. We enrolled 32 therapy-naïve CLL patients to receive ibrutinib plus obinutuzumab, followed by single-agent ibrutinib. Patients could discontinue ibrutinib after 36 months with sustained complete response (CR). We evaluated treatment safety, efficacy, and outcomes after ibrutinib discontinuation. The overall response rate was 100%, 28% achieved a CR, and 12.5% achieved bone marrow undetectable minimal residual disease. At a three-year median follow-up, 91% remain in remission with 100% overall survival. Five patients in sustained CR stopped ibrutinib and have not progressed. Eight non-CR patients discontinued for other reasons, with only two progressing. The treatment was safe, with a lower IRR rate. All patients responded to treatment with longer time-to-progression after discontinuation of ibrutinib. Our data support the evaluation of ibrutinib discontinuation strategies in more extensive clinical trials (https://Clinicaltrials.gov Identifier https://clinicaltrials.gov/ct2/show/NCT02315768).</p>","PeriodicalId":7325,"journal":{"name":"Advances in Hematology","volume":" ","pages":"4450824"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8800600/pdf/","citationCount":"2","resultStr":"{\"title\":\"Ibrutinib plus Obinutuzumab as Frontline Therapy for Chronic Lymphocytic Leukemia Is Associated with a Lower Rate of Infusion-Related Reactions and with Sustained Remissions after Ibrutinib Discontinuation: A Single-Arm, Open-Label, Phase 1b/2 Clinical Trial NCT0231576.\",\"authors\":\"Januario E Castro, Paula A Lengerke-Diaz, Juliana Velez Lujan, Michael Y Choi, Eider F Moreno-Cortes, Jose V Forero, Juan Esteban Garcia-Robledo, Chaja Jacobs, Colin McCarthy, Alaina Heinen, Carlos I Amaya-Chanaga, Thomas J Kipps\",\"doi\":\"10.1155/2022/4450824\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Ibrutinib-based therapies are costly and require continuous administration. We hypothesized combining BTK inhibition with anti-CD20 monoclonal antibodies would yield deep remissions allowing discontinuation. We enrolled 32 therapy-naïve CLL patients to receive ibrutinib plus obinutuzumab, followed by single-agent ibrutinib. Patients could discontinue ibrutinib after 36 months with sustained complete response (CR). We evaluated treatment safety, efficacy, and outcomes after ibrutinib discontinuation. The overall response rate was 100%, 28% achieved a CR, and 12.5% achieved bone marrow undetectable minimal residual disease. At a three-year median follow-up, 91% remain in remission with 100% overall survival. Five patients in sustained CR stopped ibrutinib and have not progressed. Eight non-CR patients discontinued for other reasons, with only two progressing. The treatment was safe, with a lower IRR rate. All patients responded to treatment with longer time-to-progression after discontinuation of ibrutinib. Our data support the evaluation of ibrutinib discontinuation strategies in more extensive clinical trials (https://Clinicaltrials.gov Identifier https://clinicaltrials.gov/ct2/show/NCT02315768).</p>\",\"PeriodicalId\":7325,\"journal\":{\"name\":\"Advances in Hematology\",\"volume\":\" \",\"pages\":\"4450824\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8800600/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/4450824\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/4450824","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Ibrutinib plus Obinutuzumab as Frontline Therapy for Chronic Lymphocytic Leukemia Is Associated with a Lower Rate of Infusion-Related Reactions and with Sustained Remissions after Ibrutinib Discontinuation: A Single-Arm, Open-Label, Phase 1b/2 Clinical Trial NCT0231576.
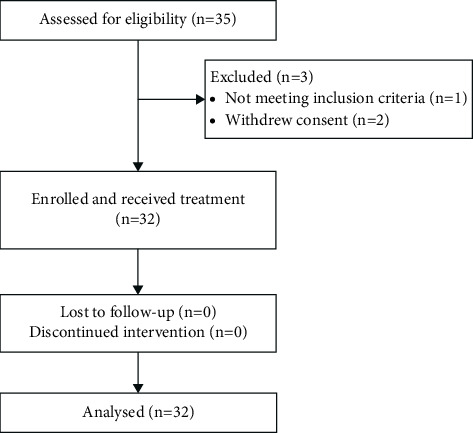
Ibrutinib-based therapies are costly and require continuous administration. We hypothesized combining BTK inhibition with anti-CD20 monoclonal antibodies would yield deep remissions allowing discontinuation. We enrolled 32 therapy-naïve CLL patients to receive ibrutinib plus obinutuzumab, followed by single-agent ibrutinib. Patients could discontinue ibrutinib after 36 months with sustained complete response (CR). We evaluated treatment safety, efficacy, and outcomes after ibrutinib discontinuation. The overall response rate was 100%, 28% achieved a CR, and 12.5% achieved bone marrow undetectable minimal residual disease. At a three-year median follow-up, 91% remain in remission with 100% overall survival. Five patients in sustained CR stopped ibrutinib and have not progressed. Eight non-CR patients discontinued for other reasons, with only two progressing. The treatment was safe, with a lower IRR rate. All patients responded to treatment with longer time-to-progression after discontinuation of ibrutinib. Our data support the evaluation of ibrutinib discontinuation strategies in more extensive clinical trials (https://Clinicaltrials.gov Identifier https://clinicaltrials.gov/ct2/show/NCT02315768).





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
