{"title":"超声引导下经腹平面阻滞用于腹腔镜妇科手术的镇痛效果:一项随机对照试验。","authors":"Divya Sethi, Garima Garg","doi":"10.17085/apm.21030","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study aimed to determine whether ultrasound-guided transversus abdominis plane (TAP) block is more effective in reducing postoperative pain and analgesic consumption than local anesthetic infiltration (LAI) at the port site for elective laparoscopic gynecological surgeries.</p><p><strong>Methods: </strong>Eighty patients with the American Society of Anesthesiologists status I/II undergoing laparoscopic gynecology surgery were enrolled for this randomized control trial. After general anesthesia was administered, patients in group C received LAI at each port site, and patients in group T received bilateral ultrasound-guided TAP. Postoperative pain was assessed at time intervals of 1/2, 2, 4, 6, 8, and 24 h using the numeric pain scale (NPS). Clinical metrics such as postoperative analgesic diclofenac consumption, need for rescue fentanyl, nausea-vomiting scores, and antiemetic requirements were also recorded.</p><p><strong>Results: </strong>Seventy-four patients were included in the final analysis. Postoperatively, patients in group T had significantly lower NPS than those in group C (P < 0.05). The highest difference in the postoperative NPS was observed at 2 h (median [1Q, 3Q]; group C = 3 [2, 4]; group T = 1 [0, 2]; P < 0.001). A statistically significant difference was observed in the frequency of diclofenac (75 mg intravenous) requirement between the groups (P = 0.010). No significant difference was observed between the groups in need of rescue fentanyl or antiemetic and the nausea-vomiting scores.</p><p><strong>Conclusions: </strong>In patients undergoing laparoscopic gynecological surgery, ultrasound-guided TAP block provided greater postoperative analgesic benefits in terms of lower NPS and reduced analgesic requirements than port site LAI.</p>","PeriodicalId":7801,"journal":{"name":"Anesthesia and pain medicine","volume":"17 1","pages":"67-74"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/76/09/apm-21030.PMC8841257.pdf","citationCount":"1","resultStr":"{\"title\":\"Analgesic efficacy of ultrasound-guided transversus abdominis plane block for laparoscopic gynecological surgery: a randomized controlled trial.\",\"authors\":\"Divya Sethi, Garima Garg\",\"doi\":\"10.17085/apm.21030\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study aimed to determine whether ultrasound-guided transversus abdominis plane (TAP) block is more effective in reducing postoperative pain and analgesic consumption than local anesthetic infiltration (LAI) at the port site for elective laparoscopic gynecological surgeries.</p><p><strong>Methods: </strong>Eighty patients with the American Society of Anesthesiologists status I/II undergoing laparoscopic gynecology surgery were enrolled for this randomized control trial. After general anesthesia was administered, patients in group C received LAI at each port site, and patients in group T received bilateral ultrasound-guided TAP. Postoperative pain was assessed at time intervals of 1/2, 2, 4, 6, 8, and 24 h using the numeric pain scale (NPS). Clinical metrics such as postoperative analgesic diclofenac consumption, need for rescue fentanyl, nausea-vomiting scores, and antiemetic requirements were also recorded.</p><p><strong>Results: </strong>Seventy-four patients were included in the final analysis. Postoperatively, patients in group T had significantly lower NPS than those in group C (P < 0.05). The highest difference in the postoperative NPS was observed at 2 h (median [1Q, 3Q]; group C = 3 [2, 4]; group T = 1 [0, 2]; P < 0.001). A statistically significant difference was observed in the frequency of diclofenac (75 mg intravenous) requirement between the groups (P = 0.010). No significant difference was observed between the groups in need of rescue fentanyl or antiemetic and the nausea-vomiting scores.</p><p><strong>Conclusions: </strong>In patients undergoing laparoscopic gynecological surgery, ultrasound-guided TAP block provided greater postoperative analgesic benefits in terms of lower NPS and reduced analgesic requirements than port site LAI.</p>\",\"PeriodicalId\":7801,\"journal\":{\"name\":\"Anesthesia and pain medicine\",\"volume\":\"17 1\",\"pages\":\"67-74\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/76/09/apm-21030.PMC8841257.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anesthesia and pain medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17085/apm.21030\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.21030","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/7 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Analgesic efficacy of ultrasound-guided transversus abdominis plane block for laparoscopic gynecological surgery: a randomized controlled trial.
Background: This study aimed to determine whether ultrasound-guided transversus abdominis plane (TAP) block is more effective in reducing postoperative pain and analgesic consumption than local anesthetic infiltration (LAI) at the port site for elective laparoscopic gynecological surgeries.
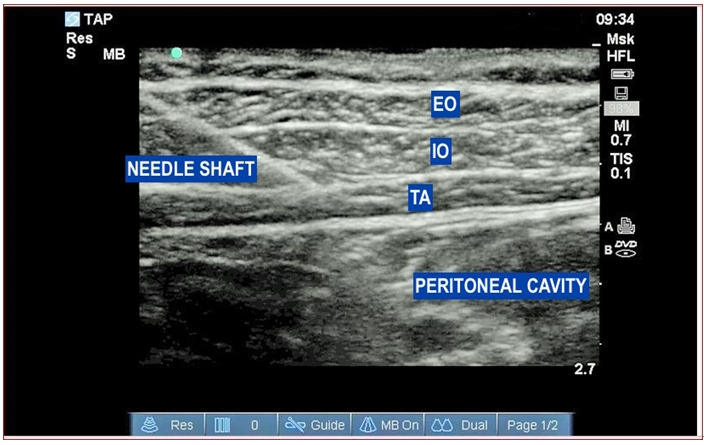
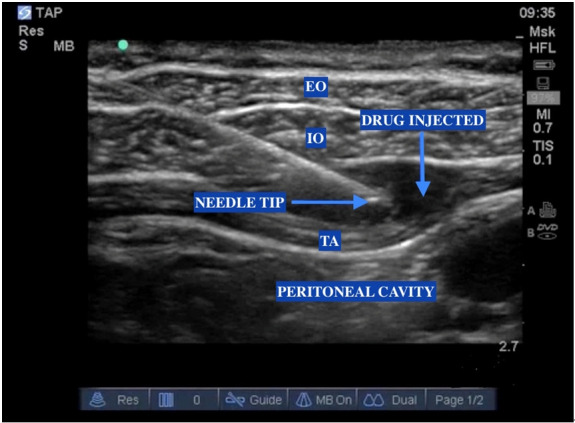
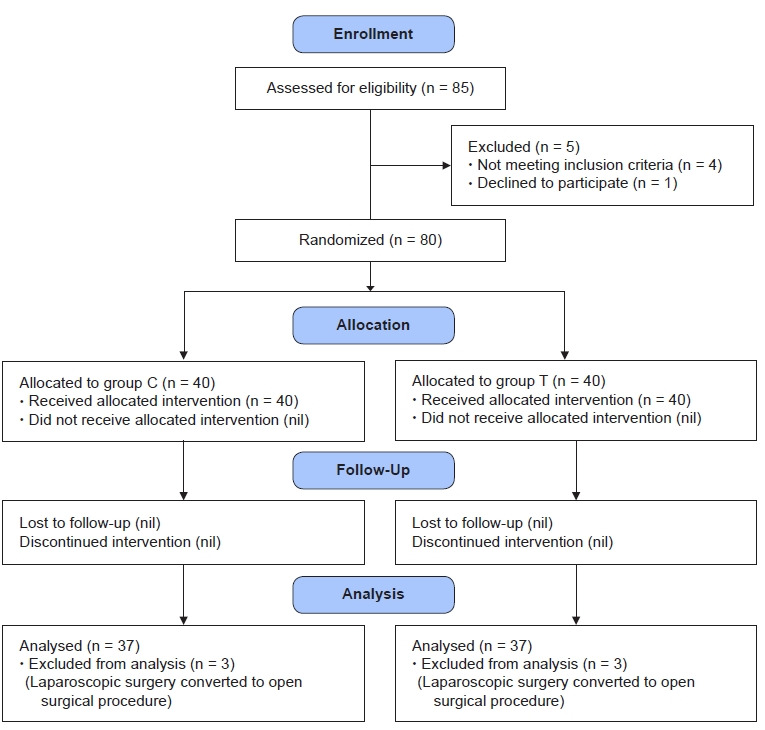
Methods: Eighty patients with the American Society of Anesthesiologists status I/II undergoing laparoscopic gynecology surgery were enrolled for this randomized control trial. After general anesthesia was administered, patients in group C received LAI at each port site, and patients in group T received bilateral ultrasound-guided TAP. Postoperative pain was assessed at time intervals of 1/2, 2, 4, 6, 8, and 24 h using the numeric pain scale (NPS). Clinical metrics such as postoperative analgesic diclofenac consumption, need for rescue fentanyl, nausea-vomiting scores, and antiemetic requirements were also recorded.
Results: Seventy-four patients were included in the final analysis. Postoperatively, patients in group T had significantly lower NPS than those in group C (P < 0.05). The highest difference in the postoperative NPS was observed at 2 h (median [1Q, 3Q]; group C = 3 [2, 4]; group T = 1 [0, 2]; P < 0.001). A statistically significant difference was observed in the frequency of diclofenac (75 mg intravenous) requirement between the groups (P = 0.010). No significant difference was observed between the groups in need of rescue fentanyl or antiemetic and the nausea-vomiting scores.
Conclusions: In patients undergoing laparoscopic gynecological surgery, ultrasound-guided TAP block provided greater postoperative analgesic benefits in terms of lower NPS and reduced analgesic requirements than port site LAI.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
