Rosalyn E. Plotzker , Gregory M. Barnell , Dorothy J. Wiley , Elizabeth A. Stier , Naomi Jay
{"title":"提供者对肛门癌预防筛查的偏好:国际肛门肿瘤协会调查的结果","authors":"Rosalyn E. Plotzker , Gregory M. Barnell , Dorothy J. Wiley , Elizabeth A. Stier , Naomi Jay","doi":"10.1016/j.tvr.2022.200235","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>This study explores provider preferences regarding anal cancer screening indications, initiation age<strong>,</strong> tools, and referral threshold to high resolution anoscopy (HRA).</p></div><div><h3>Methods</h3><p>International Anal Neoplasia Society affiliates were invited to complete an online survey. Options for initiation age and tools were delineated by sub-groups. HRA referral thresholds separately queried recommendations by patient immune status.</p></div><div><h3>Results</h3><p>One hundred forty respondents participated. Although consensus was lacking with regard to specific screening initiation age, more respondents recommended younger initiation ages for men who have sex with men (MSM) living with HIV (LWH) compared with MSM not LWH (p < 0.01). “No age threshold” ranged 44-55% among sub-groups with lower genital tract disease. Cytology and digital anorectal exam (DARE) were the most frequently selected tools for all sub-groups (ranges 77-90% and 74-86%, respectively). HRA was recommended significantly more frequently for MSM LWH (58%) and patients with vulvar cancer (52%) compared to others (p < 0.01). “Any [test] abnormality” was more often selected as indication for HRA for immunocompromised (56%) and immunocompetent (46%) patients than a specific cytology test result (29%, 36% respectively).</p></div><div><h3>Conclusion</h3><p>Cytology and DARE were preferred screening tools; screening initiation age and HRA referral threshold showed less consensus. Evidence-based guidelines are needed and may lead to more consistent screening practices.</p></div>","PeriodicalId":52381,"journal":{"name":"Tumour Virus Research","volume":"13 ","pages":"Article 200235"},"PeriodicalIF":8.1000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b5/18/main.PMC9006639.pdf","citationCount":"8","resultStr":"{\"title\":\"Provider preferences for anal cancer prevention screening: Results of the International Anal Neoplasia Society survey\",\"authors\":\"Rosalyn E. Plotzker , Gregory M. Barnell , Dorothy J. Wiley , Elizabeth A. Stier , Naomi Jay\",\"doi\":\"10.1016/j.tvr.2022.200235\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>This study explores provider preferences regarding anal cancer screening indications, initiation age<strong>,</strong> tools, and referral threshold to high resolution anoscopy (HRA).</p></div><div><h3>Methods</h3><p>International Anal Neoplasia Society affiliates were invited to complete an online survey. Options for initiation age and tools were delineated by sub-groups. HRA referral thresholds separately queried recommendations by patient immune status.</p></div><div><h3>Results</h3><p>One hundred forty respondents participated. Although consensus was lacking with regard to specific screening initiation age, more respondents recommended younger initiation ages for men who have sex with men (MSM) living with HIV (LWH) compared with MSM not LWH (p < 0.01). “No age threshold” ranged 44-55% among sub-groups with lower genital tract disease. Cytology and digital anorectal exam (DARE) were the most frequently selected tools for all sub-groups (ranges 77-90% and 74-86%, respectively). HRA was recommended significantly more frequently for MSM LWH (58%) and patients with vulvar cancer (52%) compared to others (p < 0.01). “Any [test] abnormality” was more often selected as indication for HRA for immunocompromised (56%) and immunocompetent (46%) patients than a specific cytology test result (29%, 36% respectively).</p></div><div><h3>Conclusion</h3><p>Cytology and DARE were preferred screening tools; screening initiation age and HRA referral threshold showed less consensus. Evidence-based guidelines are needed and may lead to more consistent screening practices.</p></div>\",\"PeriodicalId\":52381,\"journal\":{\"name\":\"Tumour Virus Research\",\"volume\":\"13 \",\"pages\":\"Article 200235\"},\"PeriodicalIF\":8.1000,\"publicationDate\":\"2022-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b5/18/main.PMC9006639.pdf\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tumour Virus Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666679022000015\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/2/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"VIROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tumour Virus Research","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666679022000015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/2/17 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"VIROLOGY","Score":null,"Total":0}
Provider preferences for anal cancer prevention screening: Results of the International Anal Neoplasia Society survey
Objective
This study explores provider preferences regarding anal cancer screening indications, initiation age, tools, and referral threshold to high resolution anoscopy (HRA).
Methods
International Anal Neoplasia Society affiliates were invited to complete an online survey. Options for initiation age and tools were delineated by sub-groups. HRA referral thresholds separately queried recommendations by patient immune status.
Results
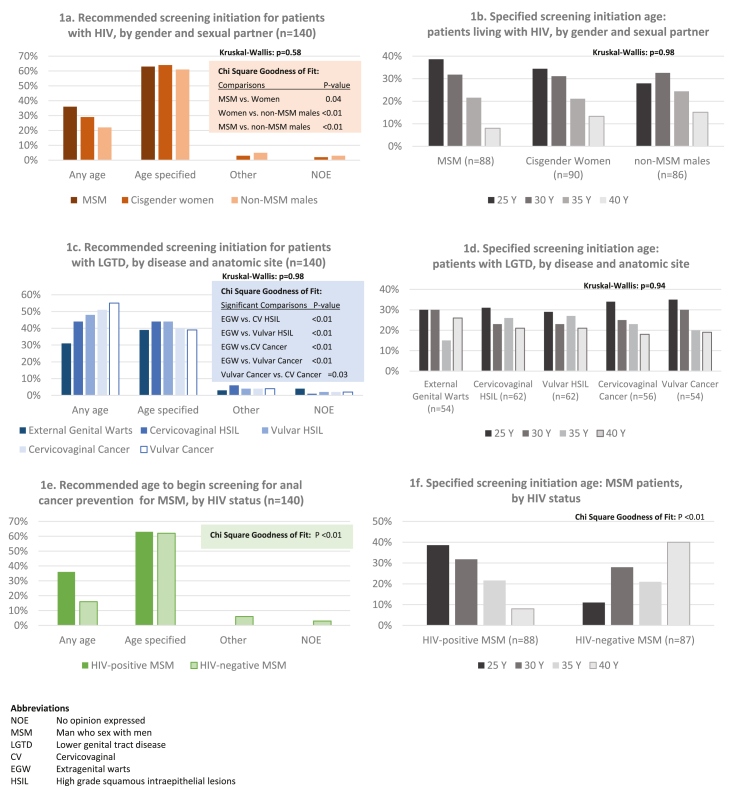
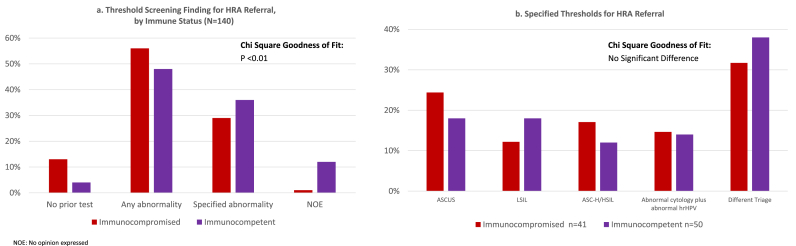
One hundred forty respondents participated. Although consensus was lacking with regard to specific screening initiation age, more respondents recommended younger initiation ages for men who have sex with men (MSM) living with HIV (LWH) compared with MSM not LWH (p < 0.01). “No age threshold” ranged 44-55% among sub-groups with lower genital tract disease. Cytology and digital anorectal exam (DARE) were the most frequently selected tools for all sub-groups (ranges 77-90% and 74-86%, respectively). HRA was recommended significantly more frequently for MSM LWH (58%) and patients with vulvar cancer (52%) compared to others (p < 0.01). “Any [test] abnormality” was more often selected as indication for HRA for immunocompromised (56%) and immunocompetent (46%) patients than a specific cytology test result (29%, 36% respectively).
Conclusion
Cytology and DARE were preferred screening tools; screening initiation age and HRA referral threshold showed less consensus. Evidence-based guidelines are needed and may lead to more consistent screening practices.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
