Nicole Young, Alison Bowman, Kjell Swedin, James Collins, Nathaniel D Blair-Stahn, Paulina A Lindstedt, Christopher Troeger, Abraham D Flaxman
{"title":"在印度、巴基斯坦、马里和坦桑尼亚,与补充铁和叶酸相比,产前补充多种微量营养素和平衡能量蛋白质的成本效益:一项动态微观模拟研究。","authors":"Nicole Young, Alison Bowman, Kjell Swedin, James Collins, Nathaniel D Blair-Stahn, Paulina A Lindstedt, Christopher Troeger, Abraham D Flaxman","doi":"10.1371/journal.pmed.1003902","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Malnutrition among women of childbearing age is especially prevalent in Asia and sub-Saharan Africa and can be harmful to the fetus during pregnancy. In the most recently available Demographic and Health Survey (DHS), approximately 10% to 20% of pregnant women in India, Pakistan, Mali, and Tanzania were undernourished (body mass index [BMI] <18.5 kg/m2), and according to the Global Burden of Disease (GBD) 2017 study, approximately 20% of babies were born with low birth weight (LBW; <2,500 g) in India, Pakistan, and Mali and 8% in Tanzania. Supplementing pregnant women with micro and macronutrients during the antenatal period can improve birth outcomes. Recently, the World Health Organization (WHO) recommended antenatal multiple micronutrient supplementation (MMS) that includes iron and folic acid (IFA) in the context of rigorous research. Additionally, WHO recommends balanced energy protein (BEP) for undernourished populations. However, few studies have compared the cost-effectiveness of different supplementation regimens. We compared the cost-effectiveness of MMS and BEP with IFA to quantify their benefits in 4 countries with considerable prevalence of maternal undernutrition.</p><p><strong>Methods and findings: </strong>Using nationally representative estimates from the 2017 GBD study, we conducted an individual-based dynamic microsimulation of population cohorts from birth to 2 years of age in India, Pakistan, Mali, and Tanzania. We modeled the effect of maternal nutritional supplementation on infant birth weight, stunting and wasting using effect sizes from Cochrane systematic reviews and published literature. We used a payer's perspective and obtained costs of supplementation per pregnancy from the published literature. We compared disability-adjusted life years (DALYs) and incremental cost-effectiveness ratios (ICERs) in a baseline scenario with existing antenatal IFA coverage with scenarios where 90% of antenatal care (ANC) attendees receive either universal MMS, universal BEP, or MMS + targeted BEP (women with prepregnancy BMI <18.5 kg/m2 receive BEP containing MMS while women with BMI ≥18.5 kg/m2 receive MMS). We obtained 95% uncertainty intervals (UIs) for all outputs to represent parameter and stochastic uncertainty across 100 iterations of model runs. ICERs for all scenarios were lowest in Pakistan and greatest in Tanzania, in line with the baseline trend in prevalence of and attributable burden to LBW. MMS + targeted BEP averts more DALYs than universal MMS alone while remaining cost-effective. ICERs for universal MMS compared to baseline IFA were $52 (95% UI: $28 to $78) for Pakistan, $72 (95% UI: $37 to $118) for Mali, $70 (95% UI: $43 to $104) for India, and $253 (95% UI: $112 to $481) for Tanzania. ICERs for MMS + targeted BEP compared to baseline IFA were $54 (95% UI: $32 to $77) for Pakistan, $73 (95% UI: $40 to $104) for Mali, $83 (95% UI: $58 to $111) for India, and $245 (95% UI: $127 to $405) for Tanzania. Study limitations include generalizing experimental findings from the literature to our populations of interest and using population-level input parameters that may not reflect the heterogeneity of subpopulations. Additionally, our microsimulation fuses multiple sources of data and may be limited by data quality and availability.</p><p><strong>Conclusions: </strong>In this study, we observed that MMS + targeted BEP averts more DALYs and remains cost-effective compared to universal MMS. As countries consider using MMS in alignment with recent WHO guidelines, offering targeted BEP is a cost-effective strategy that can be considered concurrently to maximize benefits and synergize program implementation.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 2","pages":"e1003902"},"PeriodicalIF":9.9000,"publicationDate":"2022-02-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8863292/pdf/","citationCount":"1","resultStr":"{\"title\":\"Cost-effectiveness of antenatal multiple micronutrients and balanced energy protein supplementation compared to iron and folic acid supplementation in India, Pakistan, Mali, and Tanzania: A dynamic microsimulation study.\",\"authors\":\"Nicole Young, Alison Bowman, Kjell Swedin, James Collins, Nathaniel D Blair-Stahn, Paulina A Lindstedt, Christopher Troeger, Abraham D Flaxman\",\"doi\":\"10.1371/journal.pmed.1003902\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Malnutrition among women of childbearing age is especially prevalent in Asia and sub-Saharan Africa and can be harmful to the fetus during pregnancy. In the most recently available Demographic and Health Survey (DHS), approximately 10% to 20% of pregnant women in India, Pakistan, Mali, and Tanzania were undernourished (body mass index [BMI] <18.5 kg/m2), and according to the Global Burden of Disease (GBD) 2017 study, approximately 20% of babies were born with low birth weight (LBW; <2,500 g) in India, Pakistan, and Mali and 8% in Tanzania. Supplementing pregnant women with micro and macronutrients during the antenatal period can improve birth outcomes. Recently, the World Health Organization (WHO) recommended antenatal multiple micronutrient supplementation (MMS) that includes iron and folic acid (IFA) in the context of rigorous research. Additionally, WHO recommends balanced energy protein (BEP) for undernourished populations. However, few studies have compared the cost-effectiveness of different supplementation regimens. We compared the cost-effectiveness of MMS and BEP with IFA to quantify their benefits in 4 countries with considerable prevalence of maternal undernutrition.</p><p><strong>Methods and findings: </strong>Using nationally representative estimates from the 2017 GBD study, we conducted an individual-based dynamic microsimulation of population cohorts from birth to 2 years of age in India, Pakistan, Mali, and Tanzania. We modeled the effect of maternal nutritional supplementation on infant birth weight, stunting and wasting using effect sizes from Cochrane systematic reviews and published literature. We used a payer's perspective and obtained costs of supplementation per pregnancy from the published literature. We compared disability-adjusted life years (DALYs) and incremental cost-effectiveness ratios (ICERs) in a baseline scenario with existing antenatal IFA coverage with scenarios where 90% of antenatal care (ANC) attendees receive either universal MMS, universal BEP, or MMS + targeted BEP (women with prepregnancy BMI <18.5 kg/m2 receive BEP containing MMS while women with BMI ≥18.5 kg/m2 receive MMS). We obtained 95% uncertainty intervals (UIs) for all outputs to represent parameter and stochastic uncertainty across 100 iterations of model runs. ICERs for all scenarios were lowest in Pakistan and greatest in Tanzania, in line with the baseline trend in prevalence of and attributable burden to LBW. MMS + targeted BEP averts more DALYs than universal MMS alone while remaining cost-effective. ICERs for universal MMS compared to baseline IFA were $52 (95% UI: $28 to $78) for Pakistan, $72 (95% UI: $37 to $118) for Mali, $70 (95% UI: $43 to $104) for India, and $253 (95% UI: $112 to $481) for Tanzania. ICERs for MMS + targeted BEP compared to baseline IFA were $54 (95% UI: $32 to $77) for Pakistan, $73 (95% UI: $40 to $104) for Mali, $83 (95% UI: $58 to $111) for India, and $245 (95% UI: $127 to $405) for Tanzania. Study limitations include generalizing experimental findings from the literature to our populations of interest and using population-level input parameters that may not reflect the heterogeneity of subpopulations. Additionally, our microsimulation fuses multiple sources of data and may be limited by data quality and availability.</p><p><strong>Conclusions: </strong>In this study, we observed that MMS + targeted BEP averts more DALYs and remains cost-effective compared to universal MMS. As countries consider using MMS in alignment with recent WHO guidelines, offering targeted BEP is a cost-effective strategy that can be considered concurrently to maximize benefits and synergize program implementation.</p>\",\"PeriodicalId\":20368,\"journal\":{\"name\":\"PLoS Medicine\",\"volume\":\"19 2\",\"pages\":\"e1003902\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2022-02-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8863292/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pmed.1003902\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/2/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003902","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/2/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Cost-effectiveness of antenatal multiple micronutrients and balanced energy protein supplementation compared to iron and folic acid supplementation in India, Pakistan, Mali, and Tanzania: A dynamic microsimulation study.
Background: Malnutrition among women of childbearing age is especially prevalent in Asia and sub-Saharan Africa and can be harmful to the fetus during pregnancy. In the most recently available Demographic and Health Survey (DHS), approximately 10% to 20% of pregnant women in India, Pakistan, Mali, and Tanzania were undernourished (body mass index [BMI] <18.5 kg/m2), and according to the Global Burden of Disease (GBD) 2017 study, approximately 20% of babies were born with low birth weight (LBW; <2,500 g) in India, Pakistan, and Mali and 8% in Tanzania. Supplementing pregnant women with micro and macronutrients during the antenatal period can improve birth outcomes. Recently, the World Health Organization (WHO) recommended antenatal multiple micronutrient supplementation (MMS) that includes iron and folic acid (IFA) in the context of rigorous research. Additionally, WHO recommends balanced energy protein (BEP) for undernourished populations. However, few studies have compared the cost-effectiveness of different supplementation regimens. We compared the cost-effectiveness of MMS and BEP with IFA to quantify their benefits in 4 countries with considerable prevalence of maternal undernutrition.
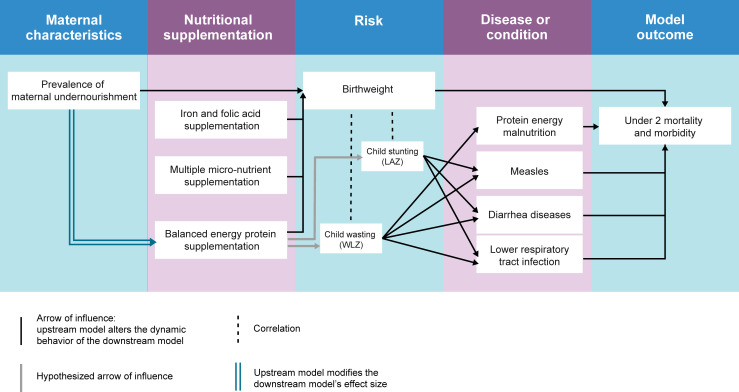
Methods and findings: Using nationally representative estimates from the 2017 GBD study, we conducted an individual-based dynamic microsimulation of population cohorts from birth to 2 years of age in India, Pakistan, Mali, and Tanzania. We modeled the effect of maternal nutritional supplementation on infant birth weight, stunting and wasting using effect sizes from Cochrane systematic reviews and published literature. We used a payer's perspective and obtained costs of supplementation per pregnancy from the published literature. We compared disability-adjusted life years (DALYs) and incremental cost-effectiveness ratios (ICERs) in a baseline scenario with existing antenatal IFA coverage with scenarios where 90% of antenatal care (ANC) attendees receive either universal MMS, universal BEP, or MMS + targeted BEP (women with prepregnancy BMI <18.5 kg/m2 receive BEP containing MMS while women with BMI ≥18.5 kg/m2 receive MMS). We obtained 95% uncertainty intervals (UIs) for all outputs to represent parameter and stochastic uncertainty across 100 iterations of model runs. ICERs for all scenarios were lowest in Pakistan and greatest in Tanzania, in line with the baseline trend in prevalence of and attributable burden to LBW. MMS + targeted BEP averts more DALYs than universal MMS alone while remaining cost-effective. ICERs for universal MMS compared to baseline IFA were $52 (95% UI: $28 to $78) for Pakistan, $72 (95% UI: $37 to $118) for Mali, $70 (95% UI: $43 to $104) for India, and $253 (95% UI: $112 to $481) for Tanzania. ICERs for MMS + targeted BEP compared to baseline IFA were $54 (95% UI: $32 to $77) for Pakistan, $73 (95% UI: $40 to $104) for Mali, $83 (95% UI: $58 to $111) for India, and $245 (95% UI: $127 to $405) for Tanzania. Study limitations include generalizing experimental findings from the literature to our populations of interest and using population-level input parameters that may not reflect the heterogeneity of subpopulations. Additionally, our microsimulation fuses multiple sources of data and may be limited by data quality and availability.
Conclusions: In this study, we observed that MMS + targeted BEP averts more DALYs and remains cost-effective compared to universal MMS. As countries consider using MMS in alignment with recent WHO guidelines, offering targeted BEP is a cost-effective strategy that can be considered concurrently to maximize benefits and synergize program implementation.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.






 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
