Amit Kaura, Adam Hartley, Vasileios Panoulas, Ben Glampson, Anoop S V Shah, Jim Davies, Abdulrahim Mulla, Kerrie Woods, Joe Omigie, Anoop D Shah, Mark R Thursz, Paul Elliott, Harry Hemmingway, Bryan Williams, Folkert W Asselbergs, Michael O'Sullivan, Graham M Lord, Adam Trickey, Jonathan Ac Sterne, Dorian O Haskard, Narbeh Melikian, Darrel P Francis, Wolfgang Koenig, Ajay M Shah, Rajesh Kharbanda, Divaka Perera, Riyaz S Patel, Keith M Channon, Jamil Mayet, Ramzi Khamis
{"title":"疑似急性冠状动脉综合征患者高敏 C 反应蛋白的死亡率风险预测:一项队列研究。","authors":"Amit Kaura, Adam Hartley, Vasileios Panoulas, Ben Glampson, Anoop S V Shah, Jim Davies, Abdulrahim Mulla, Kerrie Woods, Joe Omigie, Anoop D Shah, Mark R Thursz, Paul Elliott, Harry Hemmingway, Bryan Williams, Folkert W Asselbergs, Michael O'Sullivan, Graham M Lord, Adam Trickey, Jonathan Ac Sterne, Dorian O Haskard, Narbeh Melikian, Darrel P Francis, Wolfgang Koenig, Ajay M Shah, Rajesh Kharbanda, Divaka Perera, Riyaz S Patel, Keith M Channon, Jamil Mayet, Ramzi Khamis","doi":"10.1371/journal.pmed.1003911","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is limited evidence on the use of high-sensitivity C-reactive protein (hsCRP) as a biomarker for selecting patients for advanced cardiovascular (CV) therapies in the modern era. The prognostic value of mildly elevated hsCRP beyond troponin in a large real-world cohort of unselected patients presenting with suspected acute coronary syndrome (ACS) is unknown. We evaluated whether a mildly elevated hsCRP (up to 15 mg/L) was associated with mortality risk, beyond troponin level, in patients with suspected ACS.</p><p><strong>Methods and findings: </strong>We conducted a retrospective cohort study based on the National Institute for Health Research Health Informatics Collaborative data of 257,948 patients with suspected ACS who had a troponin measured at 5 cardiac centres in the United Kingdom between 2010 and 2017. Patients were divided into 4 hsCRP groups (<2, 2 to 4.9, 5 to 9.9, and 10 to 15 mg/L). The main outcome measure was mortality within 3 years of index presentation. The association between hsCRP levels and all-cause mortality was assessed using multivariable Cox regression analysis adjusted for age, sex, haemoglobin, white cell count (WCC), platelet count, creatinine, and troponin. Following the exclusion criteria, there were 102,337 patients included in the analysis (hsCRP <2 mg/L (n = 38,390), 2 to 4.9 mg/L (n = 27,397), 5 to 9.9 mg/L (n = 26,957), and 10 to 15 mg/L (n = 9,593)). On multivariable Cox regression analysis, there was a positive and graded relationship between hsCRP level and mortality at baseline, which remained at 3 years (hazard ratio (HR) (95% CI) of 1.32 (1.18 to 1.48) for those with hsCRP 2.0 to 4.9 mg/L and 1.40 (1.26 to 1.57) and 2.00 (1.75 to 2.28) for those with hsCRP 5 to 9.9 mg/L and 10 to 15 mg/L, respectively. This relationship was independent of troponin in all suspected ACS patients and was further verified in those who were confirmed to have an ACS diagnosis by clinical coding. The main limitation of our study is that we did not have data on underlying cause of death; however, the exclusion of those with abnormal WCC or hsCRP levels >15 mg/L makes it unlikely that sepsis was a major contributor.</p><p><strong>Conclusions: </strong>These multicentre, real-world data from a large cohort of patients with suspected ACS suggest that mildly elevated hsCRP (up to 15 mg/L) may be a clinically meaningful prognostic marker beyond troponin and point to its potential utility in selecting patients for novel treatments targeting inflammation.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov - NCT03507309.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 2","pages":"e1003911"},"PeriodicalIF":9.9000,"publicationDate":"2022-02-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8863282/pdf/","citationCount":"0","resultStr":"{\"title\":\"Mortality risk prediction of high-sensitivity C-reactive protein in suspected acute coronary syndrome: A cohort study.\",\"authors\":\"Amit Kaura, Adam Hartley, Vasileios Panoulas, Ben Glampson, Anoop S V Shah, Jim Davies, Abdulrahim Mulla, Kerrie Woods, Joe Omigie, Anoop D Shah, Mark R Thursz, Paul Elliott, Harry Hemmingway, Bryan Williams, Folkert W Asselbergs, Michael O'Sullivan, Graham M Lord, Adam Trickey, Jonathan Ac Sterne, Dorian O Haskard, Narbeh Melikian, Darrel P Francis, Wolfgang Koenig, Ajay M Shah, Rajesh Kharbanda, Divaka Perera, Riyaz S Patel, Keith M Channon, Jamil Mayet, Ramzi Khamis\",\"doi\":\"10.1371/journal.pmed.1003911\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>There is limited evidence on the use of high-sensitivity C-reactive protein (hsCRP) as a biomarker for selecting patients for advanced cardiovascular (CV) therapies in the modern era. The prognostic value of mildly elevated hsCRP beyond troponin in a large real-world cohort of unselected patients presenting with suspected acute coronary syndrome (ACS) is unknown. We evaluated whether a mildly elevated hsCRP (up to 15 mg/L) was associated with mortality risk, beyond troponin level, in patients with suspected ACS.</p><p><strong>Methods and findings: </strong>We conducted a retrospective cohort study based on the National Institute for Health Research Health Informatics Collaborative data of 257,948 patients with suspected ACS who had a troponin measured at 5 cardiac centres in the United Kingdom between 2010 and 2017. Patients were divided into 4 hsCRP groups (<2, 2 to 4.9, 5 to 9.9, and 10 to 15 mg/L). The main outcome measure was mortality within 3 years of index presentation. The association between hsCRP levels and all-cause mortality was assessed using multivariable Cox regression analysis adjusted for age, sex, haemoglobin, white cell count (WCC), platelet count, creatinine, and troponin. Following the exclusion criteria, there were 102,337 patients included in the analysis (hsCRP <2 mg/L (n = 38,390), 2 to 4.9 mg/L (n = 27,397), 5 to 9.9 mg/L (n = 26,957), and 10 to 15 mg/L (n = 9,593)). On multivariable Cox regression analysis, there was a positive and graded relationship between hsCRP level and mortality at baseline, which remained at 3 years (hazard ratio (HR) (95% CI) of 1.32 (1.18 to 1.48) for those with hsCRP 2.0 to 4.9 mg/L and 1.40 (1.26 to 1.57) and 2.00 (1.75 to 2.28) for those with hsCRP 5 to 9.9 mg/L and 10 to 15 mg/L, respectively. This relationship was independent of troponin in all suspected ACS patients and was further verified in those who were confirmed to have an ACS diagnosis by clinical coding. The main limitation of our study is that we did not have data on underlying cause of death; however, the exclusion of those with abnormal WCC or hsCRP levels >15 mg/L makes it unlikely that sepsis was a major contributor.</p><p><strong>Conclusions: </strong>These multicentre, real-world data from a large cohort of patients with suspected ACS suggest that mildly elevated hsCRP (up to 15 mg/L) may be a clinically meaningful prognostic marker beyond troponin and point to its potential utility in selecting patients for novel treatments targeting inflammation.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov - NCT03507309.</p>\",\"PeriodicalId\":20368,\"journal\":{\"name\":\"PLoS Medicine\",\"volume\":\"19 2\",\"pages\":\"e1003911\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2022-02-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8863282/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pmed.1003911\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/2/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003911","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/2/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Mortality risk prediction of high-sensitivity C-reactive protein in suspected acute coronary syndrome: A cohort study.
Background: There is limited evidence on the use of high-sensitivity C-reactive protein (hsCRP) as a biomarker for selecting patients for advanced cardiovascular (CV) therapies in the modern era. The prognostic value of mildly elevated hsCRP beyond troponin in a large real-world cohort of unselected patients presenting with suspected acute coronary syndrome (ACS) is unknown. We evaluated whether a mildly elevated hsCRP (up to 15 mg/L) was associated with mortality risk, beyond troponin level, in patients with suspected ACS.
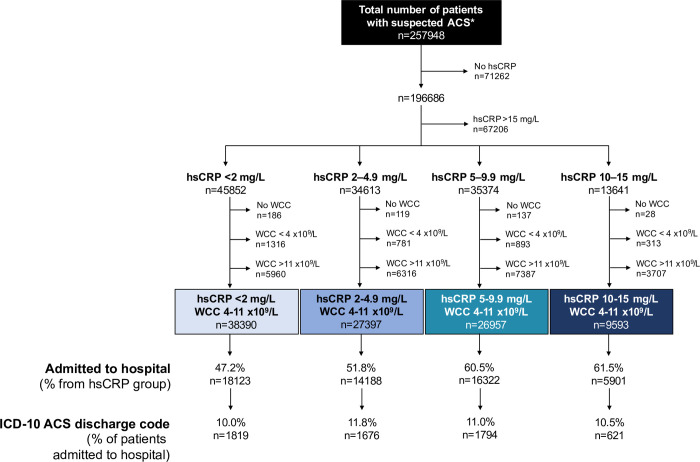
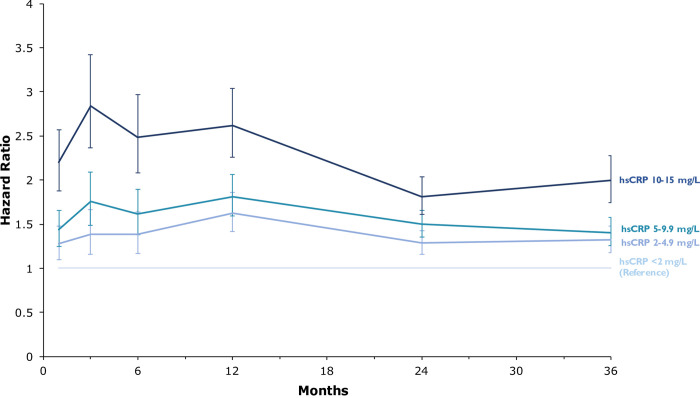
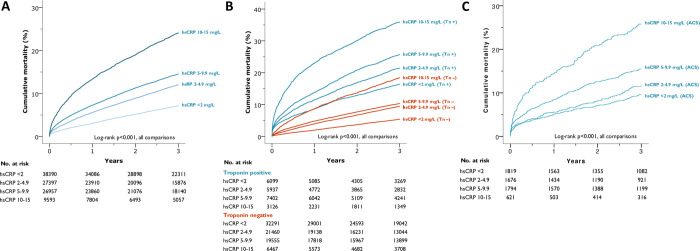
Methods and findings: We conducted a retrospective cohort study based on the National Institute for Health Research Health Informatics Collaborative data of 257,948 patients with suspected ACS who had a troponin measured at 5 cardiac centres in the United Kingdom between 2010 and 2017. Patients were divided into 4 hsCRP groups (<2, 2 to 4.9, 5 to 9.9, and 10 to 15 mg/L). The main outcome measure was mortality within 3 years of index presentation. The association between hsCRP levels and all-cause mortality was assessed using multivariable Cox regression analysis adjusted for age, sex, haemoglobin, white cell count (WCC), platelet count, creatinine, and troponin. Following the exclusion criteria, there were 102,337 patients included in the analysis (hsCRP <2 mg/L (n = 38,390), 2 to 4.9 mg/L (n = 27,397), 5 to 9.9 mg/L (n = 26,957), and 10 to 15 mg/L (n = 9,593)). On multivariable Cox regression analysis, there was a positive and graded relationship between hsCRP level and mortality at baseline, which remained at 3 years (hazard ratio (HR) (95% CI) of 1.32 (1.18 to 1.48) for those with hsCRP 2.0 to 4.9 mg/L and 1.40 (1.26 to 1.57) and 2.00 (1.75 to 2.28) for those with hsCRP 5 to 9.9 mg/L and 10 to 15 mg/L, respectively. This relationship was independent of troponin in all suspected ACS patients and was further verified in those who were confirmed to have an ACS diagnosis by clinical coding. The main limitation of our study is that we did not have data on underlying cause of death; however, the exclusion of those with abnormal WCC or hsCRP levels >15 mg/L makes it unlikely that sepsis was a major contributor.
Conclusions: These multicentre, real-world data from a large cohort of patients with suspected ACS suggest that mildly elevated hsCRP (up to 15 mg/L) may be a clinically meaningful prognostic marker beyond troponin and point to its potential utility in selecting patients for novel treatments targeting inflammation.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
