Arthur D P Mak, Sebastiaan F W Neggers, Owen N W Leung, Winnie C W Chu, Jenny Y M Ho, Idy W Y Chou, Sandra S M Chan, Linda C W Lam, Sing Lee
{"title":"低频重复经颅磁刺激治疗抗抑郁无反应双相抑郁症的抗抑郁疗效:一项单盲随机假对照试验。","authors":"Arthur D P Mak, Sebastiaan F W Neggers, Owen N W Leung, Winnie C W Chu, Jenny Y M Ho, Idy W Y Chou, Sandra S M Chan, Linda C W Lam, Sing Lee","doi":"10.1186/s40345-021-00245-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To examine the antidepressant efficacy and response predictors of R-DLPFC-LF rTMS for antidepressant-nonresponding BD.</p><p><strong>Methods: </strong>We conducted a single-blind randomized sham-controlled trial for 54 (28 sham, 26 active) patients with antidepressant-nonresponding BD (baseline MADRS ≥ 20). Patients received 15 daily sessions of active or sham neuronavigated rTMS (Figure-of-8 coil, five 1 Hz 60 s 110% RMT trains). Outcome measures included depressive response (≥ 50% MADRS reduction, CGI ≤ 2) and remission (MADRS < 7, CGI = 1) rates, treatment emergent hypo/mania (YMRS), depressive and anxiety symptoms (HAM-A).</p><p><strong>Results: </strong>48 patients (25 sham, 23 active) completed treatment, with 3 drop-outs each in active and sham groups. Active rTMS did not produce superior response or remission rates at endpoint or 6 or 12 weeks (ps > 0.05). There was no significant group * time interaction (ps > 0.05) in a multivariate ANOVA with MADRS, HAMA and YMRS as dependent variables. Exploratory analysis found MADRS improvement to be moderated by baseline anxiety (p = 0.02) and melancholia (p = 0.03) at week 3, and depressive onset at weeks 6 (p = 0.03) and 12 (p = 0.04). In subjects with below-mean anxiety (HAMA < 20.7, n = 24), MADRS improvement from active rTMS was superior to sham at week 3 (ITT, t = 2.49, p = 0.04, Cohen's d = 1.05). No seizures were observed. Groups did not differ in treatment-emergent hypomania (p = 0.1).</p><p><strong>Limitations: </strong>Larger sample size might be needed to power subgroup analyses. Moderation analyses were exploratory. Single-blind design. Unblinding before follow-up assessments due to ethical reasons.</p><p><strong>Conclusions: </strong>1-Hz 110% RMT (5 × 60 s trains) R-DLPFC-LF rTMS was not effective for antidepressant non-responding BD but may be further investigated at increased dosage and/or in BD patients with low anxiety. Trial registration CCRB Clinical Trials Registry, CUHK, CUHK_CCT00440. Registered 04 December 2014, https://www2.ccrb.cuhk.edu.hk/registry/public/279.</p>","PeriodicalId":13944,"journal":{"name":"International Journal of Bipolar Disorders","volume":"9 1","pages":"40"},"PeriodicalIF":2.8000,"publicationDate":"2021-12-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8651939/pdf/","citationCount":"3","resultStr":"{\"title\":\"Antidepressant efficacy of low-frequency repetitive transcranial magnetic stimulation in antidepressant-nonresponding bipolar depression: a single-blind randomized sham-controlled trial.\",\"authors\":\"Arthur D P Mak, Sebastiaan F W Neggers, Owen N W Leung, Winnie C W Chu, Jenny Y M Ho, Idy W Y Chou, Sandra S M Chan, Linda C W Lam, Sing Lee\",\"doi\":\"10.1186/s40345-021-00245-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>To examine the antidepressant efficacy and response predictors of R-DLPFC-LF rTMS for antidepressant-nonresponding BD.</p><p><strong>Methods: </strong>We conducted a single-blind randomized sham-controlled trial for 54 (28 sham, 26 active) patients with antidepressant-nonresponding BD (baseline MADRS ≥ 20). Patients received 15 daily sessions of active or sham neuronavigated rTMS (Figure-of-8 coil, five 1 Hz 60 s 110% RMT trains). Outcome measures included depressive response (≥ 50% MADRS reduction, CGI ≤ 2) and remission (MADRS < 7, CGI = 1) rates, treatment emergent hypo/mania (YMRS), depressive and anxiety symptoms (HAM-A).</p><p><strong>Results: </strong>48 patients (25 sham, 23 active) completed treatment, with 3 drop-outs each in active and sham groups. Active rTMS did not produce superior response or remission rates at endpoint or 6 or 12 weeks (ps > 0.05). There was no significant group * time interaction (ps > 0.05) in a multivariate ANOVA with MADRS, HAMA and YMRS as dependent variables. Exploratory analysis found MADRS improvement to be moderated by baseline anxiety (p = 0.02) and melancholia (p = 0.03) at week 3, and depressive onset at weeks 6 (p = 0.03) and 12 (p = 0.04). In subjects with below-mean anxiety (HAMA < 20.7, n = 24), MADRS improvement from active rTMS was superior to sham at week 3 (ITT, t = 2.49, p = 0.04, Cohen's d = 1.05). No seizures were observed. Groups did not differ in treatment-emergent hypomania (p = 0.1).</p><p><strong>Limitations: </strong>Larger sample size might be needed to power subgroup analyses. Moderation analyses were exploratory. Single-blind design. Unblinding before follow-up assessments due to ethical reasons.</p><p><strong>Conclusions: </strong>1-Hz 110% RMT (5 × 60 s trains) R-DLPFC-LF rTMS was not effective for antidepressant non-responding BD but may be further investigated at increased dosage and/or in BD patients with low anxiety. Trial registration CCRB Clinical Trials Registry, CUHK, CUHK_CCT00440. Registered 04 December 2014, https://www2.ccrb.cuhk.edu.hk/registry/public/279.</p>\",\"PeriodicalId\":13944,\"journal\":{\"name\":\"International Journal of Bipolar Disorders\",\"volume\":\"9 1\",\"pages\":\"40\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2021-12-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8651939/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Bipolar Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40345-021-00245-1\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PSYCHIATRY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Bipolar Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40345-021-00245-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PSYCHIATRY","Score":null,"Total":0}
Antidepressant efficacy of low-frequency repetitive transcranial magnetic stimulation in antidepressant-nonresponding bipolar depression: a single-blind randomized sham-controlled trial.
Background: To examine the antidepressant efficacy and response predictors of R-DLPFC-LF rTMS for antidepressant-nonresponding BD.
Methods: We conducted a single-blind randomized sham-controlled trial for 54 (28 sham, 26 active) patients with antidepressant-nonresponding BD (baseline MADRS ≥ 20). Patients received 15 daily sessions of active or sham neuronavigated rTMS (Figure-of-8 coil, five 1 Hz 60 s 110% RMT trains). Outcome measures included depressive response (≥ 50% MADRS reduction, CGI ≤ 2) and remission (MADRS < 7, CGI = 1) rates, treatment emergent hypo/mania (YMRS), depressive and anxiety symptoms (HAM-A).
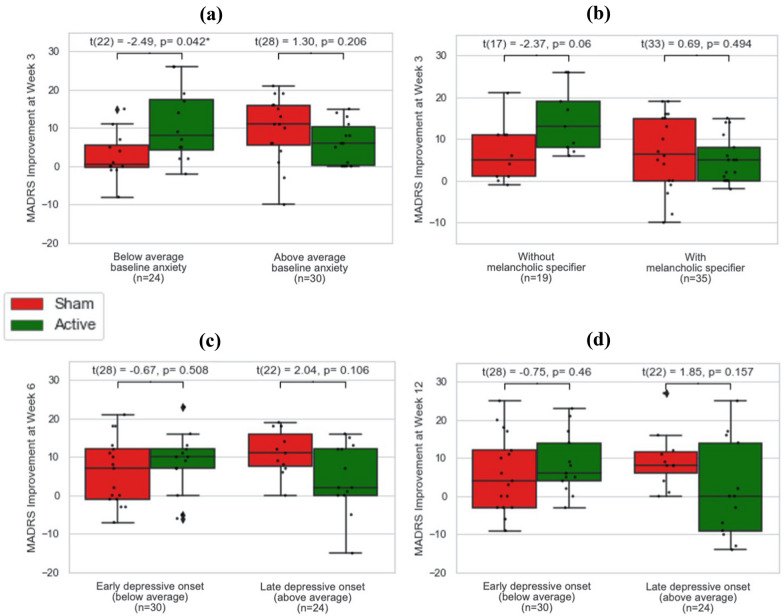
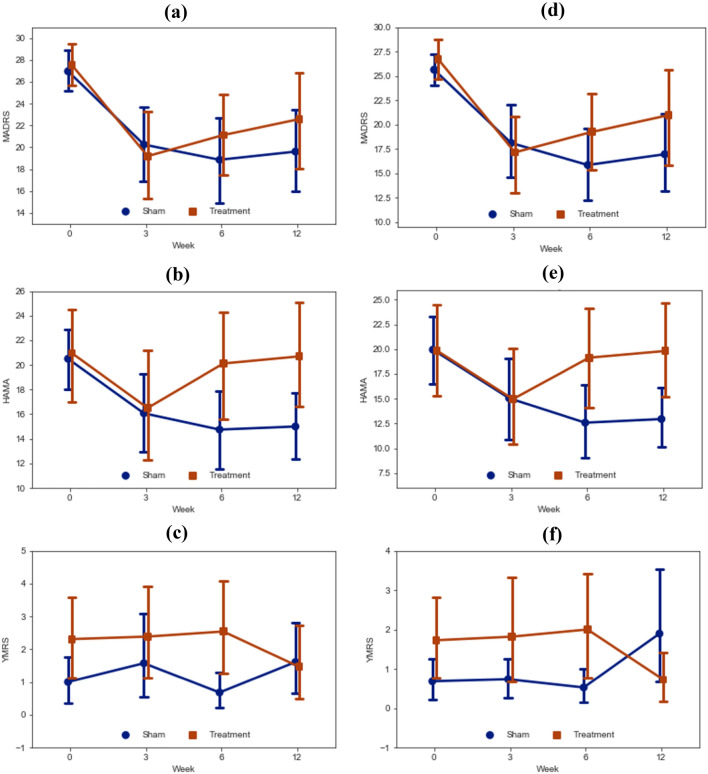
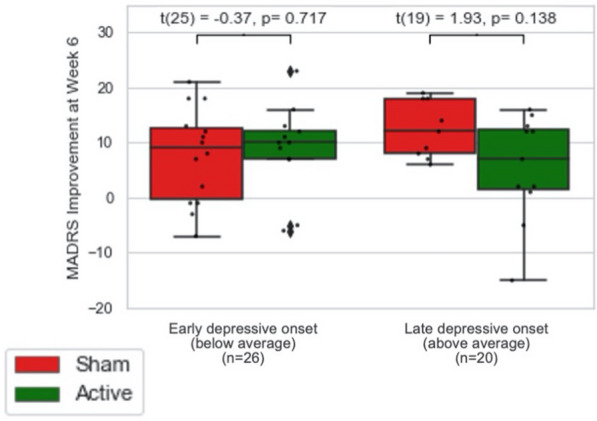
Results: 48 patients (25 sham, 23 active) completed treatment, with 3 drop-outs each in active and sham groups. Active rTMS did not produce superior response or remission rates at endpoint or 6 or 12 weeks (ps > 0.05). There was no significant group * time interaction (ps > 0.05) in a multivariate ANOVA with MADRS, HAMA and YMRS as dependent variables. Exploratory analysis found MADRS improvement to be moderated by baseline anxiety (p = 0.02) and melancholia (p = 0.03) at week 3, and depressive onset at weeks 6 (p = 0.03) and 12 (p = 0.04). In subjects with below-mean anxiety (HAMA < 20.7, n = 24), MADRS improvement from active rTMS was superior to sham at week 3 (ITT, t = 2.49, p = 0.04, Cohen's d = 1.05). No seizures were observed. Groups did not differ in treatment-emergent hypomania (p = 0.1).
Limitations: Larger sample size might be needed to power subgroup analyses. Moderation analyses were exploratory. Single-blind design. Unblinding before follow-up assessments due to ethical reasons.
Conclusions: 1-Hz 110% RMT (5 × 60 s trains) R-DLPFC-LF rTMS was not effective for antidepressant non-responding BD but may be further investigated at increased dosage and/or in BD patients with low anxiety. Trial registration CCRB Clinical Trials Registry, CUHK, CUHK_CCT00440. Registered 04 December 2014, https://www2.ccrb.cuhk.edu.hk/registry/public/279.
期刊介绍:
The International Journal of Bipolar Disorders is a peer-reviewed, open access online journal published under the SpringerOpen brand. It publishes contributions from the broad range of clinical, psychological and biological research in bipolar disorders. It is the official journal of the ECNP-ENBREC (European Network of Bipolar Research Expert Centres ) Bipolar Disorders Network, the International Group for the study of Lithium Treated Patients (IGSLi) and the Deutsche Gesellschaft für Bipolare Störungen (DGBS) and invites clinicians and researchers from around the globe to submit original research papers, short research communications, reviews, guidelines, case reports and letters to the editor that help to enhance understanding of bipolar disorders.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
