Amir Sariaslan, Michael Sharpe, Henrik Larsson, Achim Wolf, Paul Lichtenstein, Seena Fazel
{"title":"瑞典慢性呼吸系统疾病、心血管疾病和糖尿病患者的精神共病和过早死亡和自杀风险:一项超过100万患者及其未受影响的兄弟姐妹的全国匹配队列研究","authors":"Amir Sariaslan, Michael Sharpe, Henrik Larsson, Achim Wolf, Paul Lichtenstein, Seena Fazel","doi":"10.1371/journal.pmed.1003864","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Persons with noncommunicable diseases have elevated rates of premature mortality. The contribution of psychiatric comorbidity to this is uncertain. We aimed to determine the risks of premature mortality and suicide in people with common noncommunicable diseases, with and without psychiatric disorder comorbidity.</p><p><strong>Methods and findings: </strong>We used nationwide registries to study all individuals born in Sweden between 1932 and 1995 with inpatient and outpatient diagnoses of chronic respiratory diseases (n = 249,825), cardiovascular diseases (n = 568,818), and diabetes (n = 255,579) for risks of premature mortality (≤age 65 years) and suicide until 31 December 2013. Patients diagnosed with either chronic respiratory diseases, cardiovascular diseases, or diabetes were compared with age and sex-matched population controls (n = 10,345,758) and unaffected biological full siblings (n = 1,119,543). Comorbidity with any psychiatric disorder, and by major psychiatric categories, was examined using diagnoses from patient registers. Associations were quantified using stratified Cox regression models that accounted for time at risk, measured sociodemographic factors, and unmeasured familial confounders via sibling comparisons. Within 5 years of diagnosis, at least 7% (range 7.4% to 10.8%; P < 0.001) of patients with respiratory diseases, cardiovascular diseases, or diabetes (median age at diagnosis: 48 to 54 years) had died from any cause, and 0.3% (0.3% to 0.3%; P < 0.001) had died from suicide, 25% to 32% of people with these medical conditions had co-occurring lifetime diagnoses of any psychiatric disorder, most of which antedated the medical diagnosis. Comorbid psychiatric disorders were associated with higher all-cause mortality (15.4% to 21.1%) when compared to those without such conditions (5.5% to 9.1%). Suicide mortality was also elevated (1.2% to 1.6% in comorbid patients versus 0.1% to 0.1% without comorbidity). When we compared relative risks with siblings without noncommunicable diseases and psychiatric disorders, the comorbidity with any psychiatric disorder was associated with substantially increased mortality rates (adjusted HR range: aHRCR = 7.2 [95% CI: 6.8 to 7.7; P < 0.001] to aHRCV = 8.9 [95% CI: 8.5 to 9.4; P < 0.001]). Notably, comorbid substance use disorders were associated with a higher mortality rate (aHR range: aHRCR = 8.3 [95% CI: 7.6 to 9.1; P < 0.001] to aHRCV = 9.9 [95% CI: 9.3 to 10.6; P < 0.001]) than depression (aHR range: aHRCR = 5.3 [95% CI: 4.7 to 5.9; P < 0.001] to aHRCV = 7.4 [95% CI: 7.0 to 7.9; P < 0.001]), but risks of suicide were similar for these 2 psychiatric comorbidities. One limitation is that we relied on secondary care data to assess psychiatric comorbidities, which may have led to missing some patients with less severe comorbidities. Residual genetic confounding is another limitation, given that biological full siblings share an average of half of their cosegregating genes. However, the reported associations remained large even after adjustment for shared and unmeasured familial confounders.</p><p><strong>Conclusions: </strong>In this longitudinal study of over 1 million patients with chronic health diseases, we observed increased risks of all-cause and suicide mortality in individuals with psychiatric comorbidities. Improving assessment, treatment, and follow-up of people with comorbid psychiatric disorders may reduce the risk of mortality in people with chronic noncommunicable diseases.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 1","pages":"e1003864"},"PeriodicalIF":9.9000,"publicationDate":"2022-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8794193/pdf/","citationCount":"5","resultStr":"{\"title\":\"Psychiatric comorbidity and risk of premature mortality and suicide among those with chronic respiratory diseases, cardiovascular diseases, and diabetes in Sweden: A nationwide matched cohort study of over 1 million patients and their unaffected siblings.\",\"authors\":\"Amir Sariaslan, Michael Sharpe, Henrik Larsson, Achim Wolf, Paul Lichtenstein, Seena Fazel\",\"doi\":\"10.1371/journal.pmed.1003864\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Persons with noncommunicable diseases have elevated rates of premature mortality. The contribution of psychiatric comorbidity to this is uncertain. We aimed to determine the risks of premature mortality and suicide in people with common noncommunicable diseases, with and without psychiatric disorder comorbidity.</p><p><strong>Methods and findings: </strong>We used nationwide registries to study all individuals born in Sweden between 1932 and 1995 with inpatient and outpatient diagnoses of chronic respiratory diseases (n = 249,825), cardiovascular diseases (n = 568,818), and diabetes (n = 255,579) for risks of premature mortality (≤age 65 years) and suicide until 31 December 2013. Patients diagnosed with either chronic respiratory diseases, cardiovascular diseases, or diabetes were compared with age and sex-matched population controls (n = 10,345,758) and unaffected biological full siblings (n = 1,119,543). Comorbidity with any psychiatric disorder, and by major psychiatric categories, was examined using diagnoses from patient registers. Associations were quantified using stratified Cox regression models that accounted for time at risk, measured sociodemographic factors, and unmeasured familial confounders via sibling comparisons. Within 5 years of diagnosis, at least 7% (range 7.4% to 10.8%; P < 0.001) of patients with respiratory diseases, cardiovascular diseases, or diabetes (median age at diagnosis: 48 to 54 years) had died from any cause, and 0.3% (0.3% to 0.3%; P < 0.001) had died from suicide, 25% to 32% of people with these medical conditions had co-occurring lifetime diagnoses of any psychiatric disorder, most of which antedated the medical diagnosis. Comorbid psychiatric disorders were associated with higher all-cause mortality (15.4% to 21.1%) when compared to those without such conditions (5.5% to 9.1%). Suicide mortality was also elevated (1.2% to 1.6% in comorbid patients versus 0.1% to 0.1% without comorbidity). When we compared relative risks with siblings without noncommunicable diseases and psychiatric disorders, the comorbidity with any psychiatric disorder was associated with substantially increased mortality rates (adjusted HR range: aHRCR = 7.2 [95% CI: 6.8 to 7.7; P < 0.001] to aHRCV = 8.9 [95% CI: 8.5 to 9.4; P < 0.001]). Notably, comorbid substance use disorders were associated with a higher mortality rate (aHR range: aHRCR = 8.3 [95% CI: 7.6 to 9.1; P < 0.001] to aHRCV = 9.9 [95% CI: 9.3 to 10.6; P < 0.001]) than depression (aHR range: aHRCR = 5.3 [95% CI: 4.7 to 5.9; P < 0.001] to aHRCV = 7.4 [95% CI: 7.0 to 7.9; P < 0.001]), but risks of suicide were similar for these 2 psychiatric comorbidities. One limitation is that we relied on secondary care data to assess psychiatric comorbidities, which may have led to missing some patients with less severe comorbidities. Residual genetic confounding is another limitation, given that biological full siblings share an average of half of their cosegregating genes. However, the reported associations remained large even after adjustment for shared and unmeasured familial confounders.</p><p><strong>Conclusions: </strong>In this longitudinal study of over 1 million patients with chronic health diseases, we observed increased risks of all-cause and suicide mortality in individuals with psychiatric comorbidities. Improving assessment, treatment, and follow-up of people with comorbid psychiatric disorders may reduce the risk of mortality in people with chronic noncommunicable diseases.</p>\",\"PeriodicalId\":20368,\"journal\":{\"name\":\"PLoS Medicine\",\"volume\":\"19 1\",\"pages\":\"e1003864\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2022-01-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8794193/pdf/\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pmed.1003864\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003864","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Psychiatric comorbidity and risk of premature mortality and suicide among those with chronic respiratory diseases, cardiovascular diseases, and diabetes in Sweden: A nationwide matched cohort study of over 1 million patients and their unaffected siblings.
Background: Persons with noncommunicable diseases have elevated rates of premature mortality. The contribution of psychiatric comorbidity to this is uncertain. We aimed to determine the risks of premature mortality and suicide in people with common noncommunicable diseases, with and without psychiatric disorder comorbidity.
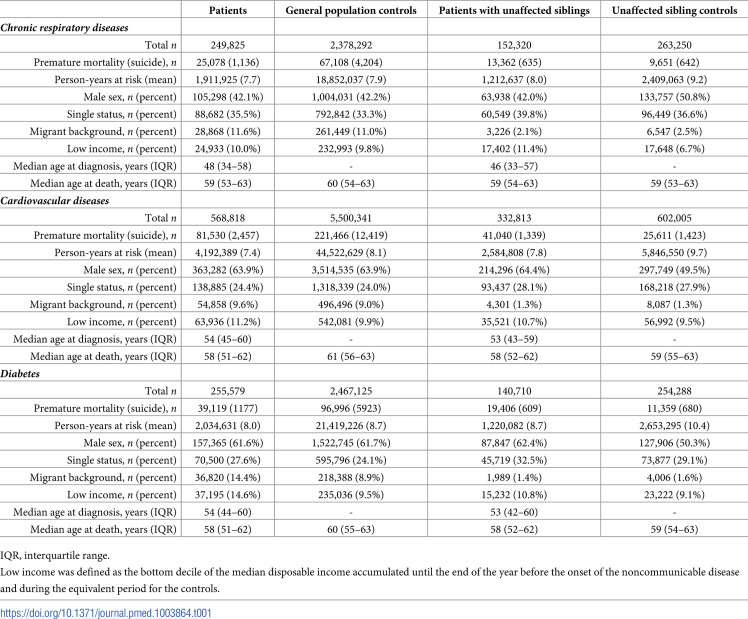
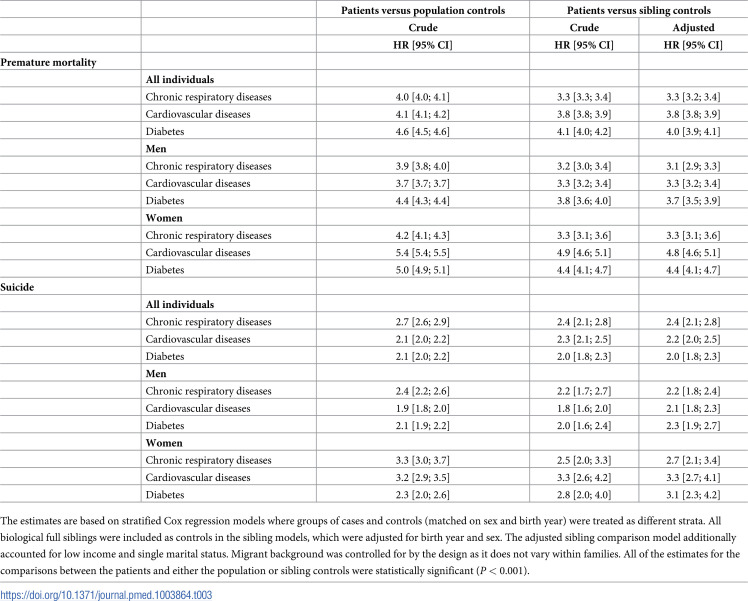
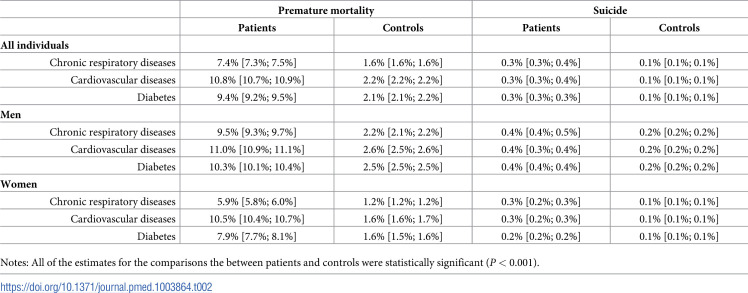
Methods and findings: We used nationwide registries to study all individuals born in Sweden between 1932 and 1995 with inpatient and outpatient diagnoses of chronic respiratory diseases (n = 249,825), cardiovascular diseases (n = 568,818), and diabetes (n = 255,579) for risks of premature mortality (≤age 65 years) and suicide until 31 December 2013. Patients diagnosed with either chronic respiratory diseases, cardiovascular diseases, or diabetes were compared with age and sex-matched population controls (n = 10,345,758) and unaffected biological full siblings (n = 1,119,543). Comorbidity with any psychiatric disorder, and by major psychiatric categories, was examined using diagnoses from patient registers. Associations were quantified using stratified Cox regression models that accounted for time at risk, measured sociodemographic factors, and unmeasured familial confounders via sibling comparisons. Within 5 years of diagnosis, at least 7% (range 7.4% to 10.8%; P < 0.001) of patients with respiratory diseases, cardiovascular diseases, or diabetes (median age at diagnosis: 48 to 54 years) had died from any cause, and 0.3% (0.3% to 0.3%; P < 0.001) had died from suicide, 25% to 32% of people with these medical conditions had co-occurring lifetime diagnoses of any psychiatric disorder, most of which antedated the medical diagnosis. Comorbid psychiatric disorders were associated with higher all-cause mortality (15.4% to 21.1%) when compared to those without such conditions (5.5% to 9.1%). Suicide mortality was also elevated (1.2% to 1.6% in comorbid patients versus 0.1% to 0.1% without comorbidity). When we compared relative risks with siblings without noncommunicable diseases and psychiatric disorders, the comorbidity with any psychiatric disorder was associated with substantially increased mortality rates (adjusted HR range: aHRCR = 7.2 [95% CI: 6.8 to 7.7; P < 0.001] to aHRCV = 8.9 [95% CI: 8.5 to 9.4; P < 0.001]). Notably, comorbid substance use disorders were associated with a higher mortality rate (aHR range: aHRCR = 8.3 [95% CI: 7.6 to 9.1; P < 0.001] to aHRCV = 9.9 [95% CI: 9.3 to 10.6; P < 0.001]) than depression (aHR range: aHRCR = 5.3 [95% CI: 4.7 to 5.9; P < 0.001] to aHRCV = 7.4 [95% CI: 7.0 to 7.9; P < 0.001]), but risks of suicide were similar for these 2 psychiatric comorbidities. One limitation is that we relied on secondary care data to assess psychiatric comorbidities, which may have led to missing some patients with less severe comorbidities. Residual genetic confounding is another limitation, given that biological full siblings share an average of half of their cosegregating genes. However, the reported associations remained large even after adjustment for shared and unmeasured familial confounders.
Conclusions: In this longitudinal study of over 1 million patients with chronic health diseases, we observed increased risks of all-cause and suicide mortality in individuals with psychiatric comorbidities. Improving assessment, treatment, and follow-up of people with comorbid psychiatric disorders may reduce the risk of mortality in people with chronic noncommunicable diseases.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
