Yue-Houng Hu, Riley H Harper, Noelle C Deiter, Jaden D Evans, Anita Mahajan, Jon J Kruse, Daniel W Mundy
{"title":"点扫描质子治疗中重新计划率的分析。","authors":"Yue-Houng Hu, Riley H Harper, Noelle C Deiter, Jaden D Evans, Anita Mahajan, Jon J Kruse, Daniel W Mundy","doi":"10.14338/IJPT-21-00043.1","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Finite proton range affords improved dose conformality of radiation therapy when patient regions-of-interest geometries are well characterized. Substantial changes in patient anatomy necessitate re-planning (RP) to maintain effective, safe treatment. Regularly planned verification scanning (VS) is performed to ensure consistent treatment quality. Substantial resources, however, are required to conduct an effective proton plan verification program, which includes but is not limited to, additional computed tomography (CT) scanner time and dedicated personnel: radiation therapists, medical physicists, physicians, and medical dosimetrists.</p><p><strong>Materials and methods: </strong>Verification scans (VSs) and re-plans (RPs) of 711 patients treated with proton therapy between June 2015 and June 2018 were studied. All treatment RP was performed with the intent to maintain original plan integrity and coverage. The treatments were classified by anatomic site: brain, craniospinal, bone, spine, head and neck (H&N), lung or chest, breast, prostate, rectum, anus, pelvis, esophagus, liver, abdomen, and extremity. Within each group, the dates of initial simulation scan, number of VSs, number of fractions completed at the time of VS, and the frequency of RP were collected. Data were analyzed in terms of rate of RP and individual likelihood of RP.</p><p><strong>Results: </strong>A total of 2196 VSs and 201 RPs were performed across all treatment sites. H&N and lung or chest disease sites represented the largest proportion of plan modifications in terms of rate of re-plan (RoR: 54% and 58%, respectively) and individual likelihood of RP on a per patient basis (likelihood of RP [RP%]: 46% and 39%, respectively). These sites required RP beyond 4 weeks of treatment, suggesting continued benefit for frequent, periodic VS. Disease sites in the lower pelvis demonstrated a low yield for RP per VS (0.01-0.02), suggesting that decreasing VS frequency, particularly late in treatment, may be reasonable.</p><p><strong>Conclusions: </strong>A large degree of variation in RoR and individual RP% was observed between anatomic treatment sites. The present retrospective analysis provides data to help develop anatomic site-based VS protocols.</p>","PeriodicalId":36923,"journal":{"name":"International Journal of Particle Therapy","volume":"9 2","pages":"49-58"},"PeriodicalIF":2.0000,"publicationDate":"2022-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9415746/pdf/","citationCount":"1","resultStr":"{\"title\":\"Analysis of the Rate of Re-planning in Spot-Scanning Proton Therapy.\",\"authors\":\"Yue-Houng Hu, Riley H Harper, Noelle C Deiter, Jaden D Evans, Anita Mahajan, Jon J Kruse, Daniel W Mundy\",\"doi\":\"10.14338/IJPT-21-00043.1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Finite proton range affords improved dose conformality of radiation therapy when patient regions-of-interest geometries are well characterized. Substantial changes in patient anatomy necessitate re-planning (RP) to maintain effective, safe treatment. Regularly planned verification scanning (VS) is performed to ensure consistent treatment quality. Substantial resources, however, are required to conduct an effective proton plan verification program, which includes but is not limited to, additional computed tomography (CT) scanner time and dedicated personnel: radiation therapists, medical physicists, physicians, and medical dosimetrists.</p><p><strong>Materials and methods: </strong>Verification scans (VSs) and re-plans (RPs) of 711 patients treated with proton therapy between June 2015 and June 2018 were studied. All treatment RP was performed with the intent to maintain original plan integrity and coverage. The treatments were classified by anatomic site: brain, craniospinal, bone, spine, head and neck (H&N), lung or chest, breast, prostate, rectum, anus, pelvis, esophagus, liver, abdomen, and extremity. Within each group, the dates of initial simulation scan, number of VSs, number of fractions completed at the time of VS, and the frequency of RP were collected. Data were analyzed in terms of rate of RP and individual likelihood of RP.</p><p><strong>Results: </strong>A total of 2196 VSs and 201 RPs were performed across all treatment sites. H&N and lung or chest disease sites represented the largest proportion of plan modifications in terms of rate of re-plan (RoR: 54% and 58%, respectively) and individual likelihood of RP on a per patient basis (likelihood of RP [RP%]: 46% and 39%, respectively). These sites required RP beyond 4 weeks of treatment, suggesting continued benefit for frequent, periodic VS. Disease sites in the lower pelvis demonstrated a low yield for RP per VS (0.01-0.02), suggesting that decreasing VS frequency, particularly late in treatment, may be reasonable.</p><p><strong>Conclusions: </strong>A large degree of variation in RoR and individual RP% was observed between anatomic treatment sites. The present retrospective analysis provides data to help develop anatomic site-based VS protocols.</p>\",\"PeriodicalId\":36923,\"journal\":{\"name\":\"International Journal of Particle Therapy\",\"volume\":\"9 2\",\"pages\":\"49-58\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2022-06-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9415746/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Particle Therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14338/IJPT-21-00043.1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Particle Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14338/IJPT-21-00043.1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Analysis of the Rate of Re-planning in Spot-Scanning Proton Therapy.
Purpose: Finite proton range affords improved dose conformality of radiation therapy when patient regions-of-interest geometries are well characterized. Substantial changes in patient anatomy necessitate re-planning (RP) to maintain effective, safe treatment. Regularly planned verification scanning (VS) is performed to ensure consistent treatment quality. Substantial resources, however, are required to conduct an effective proton plan verification program, which includes but is not limited to, additional computed tomography (CT) scanner time and dedicated personnel: radiation therapists, medical physicists, physicians, and medical dosimetrists.
Materials and methods: Verification scans (VSs) and re-plans (RPs) of 711 patients treated with proton therapy between June 2015 and June 2018 were studied. All treatment RP was performed with the intent to maintain original plan integrity and coverage. The treatments were classified by anatomic site: brain, craniospinal, bone, spine, head and neck (H&N), lung or chest, breast, prostate, rectum, anus, pelvis, esophagus, liver, abdomen, and extremity. Within each group, the dates of initial simulation scan, number of VSs, number of fractions completed at the time of VS, and the frequency of RP were collected. Data were analyzed in terms of rate of RP and individual likelihood of RP.
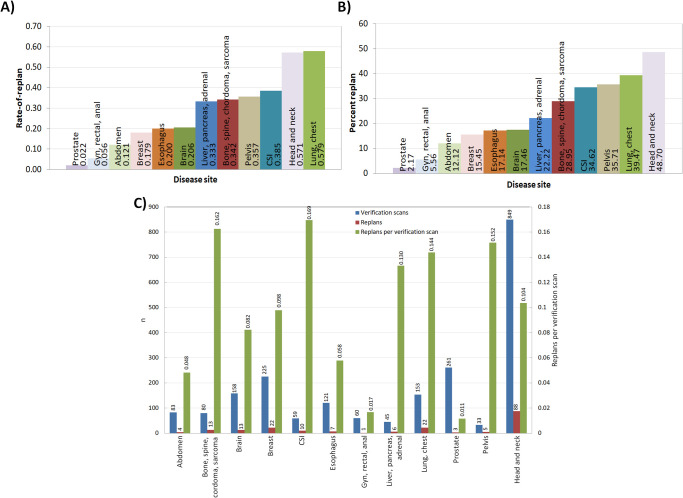
Results: A total of 2196 VSs and 201 RPs were performed across all treatment sites. H&N and lung or chest disease sites represented the largest proportion of plan modifications in terms of rate of re-plan (RoR: 54% and 58%, respectively) and individual likelihood of RP on a per patient basis (likelihood of RP [RP%]: 46% and 39%, respectively). These sites required RP beyond 4 weeks of treatment, suggesting continued benefit for frequent, periodic VS. Disease sites in the lower pelvis demonstrated a low yield for RP per VS (0.01-0.02), suggesting that decreasing VS frequency, particularly late in treatment, may be reasonable.
Conclusions: A large degree of variation in RoR and individual RP% was observed between anatomic treatment sites. The present retrospective analysis provides data to help develop anatomic site-based VS protocols.






 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
