Paola Roldan, Sriram Ravi, James Hodovan, J Todd Belcik, Stephen B Heitner, Ahmad Masri, Jonathan R Lindner
{"title":"肥厚性心肌病灌注异常的心肌超声造影评价。","authors":"Paola Roldan, Sriram Ravi, James Hodovan, J Todd Belcik, Stephen B Heitner, Ahmad Masri, Jonathan R Lindner","doi":"10.1186/s12947-022-00293-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Perfusion defects during stress can occur in hypertrophic cardiomyopathy (HCM) from either structural or functional abnormalities of the coronary microcirculation. In this study, vasodilator stress myocardial contrast echocardiography (MCE) was used to quantify and spatially characterize hyperemic myocardial blood flow (MBF) deficits in HCM.</p><p><strong>Methods: </strong>Regadenoson stress MCE was performed in patients with septal-variant HCM (n = 17) and healthy control subjects (n = 15). The presence and spatial distribution (transmural diffuse, patchy, subendocardial) of perfusion defects was determined by semiquantitative analysis. Kinetic analysis of time-intensity data was used to quantify MBF, microvascular flux rate (β), and microvascular blood volume. In patients undergoing septal myectomy (n = 3), MCE was repeated > 1 years after surgery. RESULTS: In HCM subjects, perfusion defects during stress occurred in the septum in 80%, and in non-hypertrophied regions in 40%. The majority of septal defects (83%) were patchy or subendocardial, while 67% of non-hypertrophied defects were transmural and diffuse. On quantitative analysis, hyperemic MBF was approximately 50% lower (p < 0.001) in the hypertrophied and non-hypertrophied regions of those with HCM compared to controls, largely based on an inability to augment β, although hypertrophic regions also had blood volume deficits. There was no correlation between hyperemic MBF and either percent fibrosis on magnetic resonance imaging or outflow gradient, yet those with higher degrees of fibrosis (≥ 5%) or severe gradients all had low septal MBF during regadenoson. Substantial improvement in hyperemic MBF was observed in two of the three subjects undergoing myectomy, both of whom had severe pre-surgical outflow gradients at rest.</p><p><strong>Conclusion: </strong>Perfusion defects on vasodilator MCE are common in HCM, particularly in those with extensive fibrosis, but have a different spatial pattern for the hypertrophied and non-hypertrophied segments, likely reflecting different contributions of functional and structural abnormalities. Improvement in hyperemic perfusion is possible in those undergoing septal myectomy to relieve obstruction. TRIAL REGISTRATION: ClinicalTrials.gov NCT02560467.</p>","PeriodicalId":9613,"journal":{"name":"Cardiovascular Ultrasound","volume":" ","pages":"23"},"PeriodicalIF":1.6000,"publicationDate":"2022-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9484161/pdf/","citationCount":"4","resultStr":"{\"title\":\"Myocardial contrast echocardiography assessment of perfusion abnormalities in hypertrophic cardiomyopathy.\",\"authors\":\"Paola Roldan, Sriram Ravi, James Hodovan, J Todd Belcik, Stephen B Heitner, Ahmad Masri, Jonathan R Lindner\",\"doi\":\"10.1186/s12947-022-00293-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Perfusion defects during stress can occur in hypertrophic cardiomyopathy (HCM) from either structural or functional abnormalities of the coronary microcirculation. In this study, vasodilator stress myocardial contrast echocardiography (MCE) was used to quantify and spatially characterize hyperemic myocardial blood flow (MBF) deficits in HCM.</p><p><strong>Methods: </strong>Regadenoson stress MCE was performed in patients with septal-variant HCM (n = 17) and healthy control subjects (n = 15). The presence and spatial distribution (transmural diffuse, patchy, subendocardial) of perfusion defects was determined by semiquantitative analysis. Kinetic analysis of time-intensity data was used to quantify MBF, microvascular flux rate (β), and microvascular blood volume. In patients undergoing septal myectomy (n = 3), MCE was repeated > 1 years after surgery. RESULTS: In HCM subjects, perfusion defects during stress occurred in the septum in 80%, and in non-hypertrophied regions in 40%. The majority of septal defects (83%) were patchy or subendocardial, while 67% of non-hypertrophied defects were transmural and diffuse. On quantitative analysis, hyperemic MBF was approximately 50% lower (p < 0.001) in the hypertrophied and non-hypertrophied regions of those with HCM compared to controls, largely based on an inability to augment β, although hypertrophic regions also had blood volume deficits. There was no correlation between hyperemic MBF and either percent fibrosis on magnetic resonance imaging or outflow gradient, yet those with higher degrees of fibrosis (≥ 5%) or severe gradients all had low septal MBF during regadenoson. Substantial improvement in hyperemic MBF was observed in two of the three subjects undergoing myectomy, both of whom had severe pre-surgical outflow gradients at rest.</p><p><strong>Conclusion: </strong>Perfusion defects on vasodilator MCE are common in HCM, particularly in those with extensive fibrosis, but have a different spatial pattern for the hypertrophied and non-hypertrophied segments, likely reflecting different contributions of functional and structural abnormalities. Improvement in hyperemic perfusion is possible in those undergoing septal myectomy to relieve obstruction. TRIAL REGISTRATION: ClinicalTrials.gov NCT02560467.</p>\",\"PeriodicalId\":9613,\"journal\":{\"name\":\"Cardiovascular Ultrasound\",\"volume\":\" \",\"pages\":\"23\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2022-09-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9484161/pdf/\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiovascular Ultrasound\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12947-022-00293-2\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Ultrasound","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12947-022-00293-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Myocardial contrast echocardiography assessment of perfusion abnormalities in hypertrophic cardiomyopathy.
Background: Perfusion defects during stress can occur in hypertrophic cardiomyopathy (HCM) from either structural or functional abnormalities of the coronary microcirculation. In this study, vasodilator stress myocardial contrast echocardiography (MCE) was used to quantify and spatially characterize hyperemic myocardial blood flow (MBF) deficits in HCM.
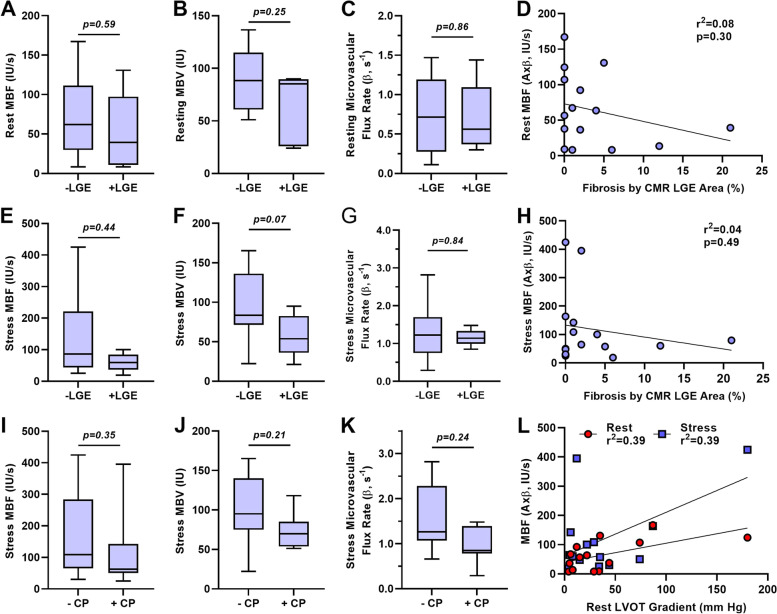
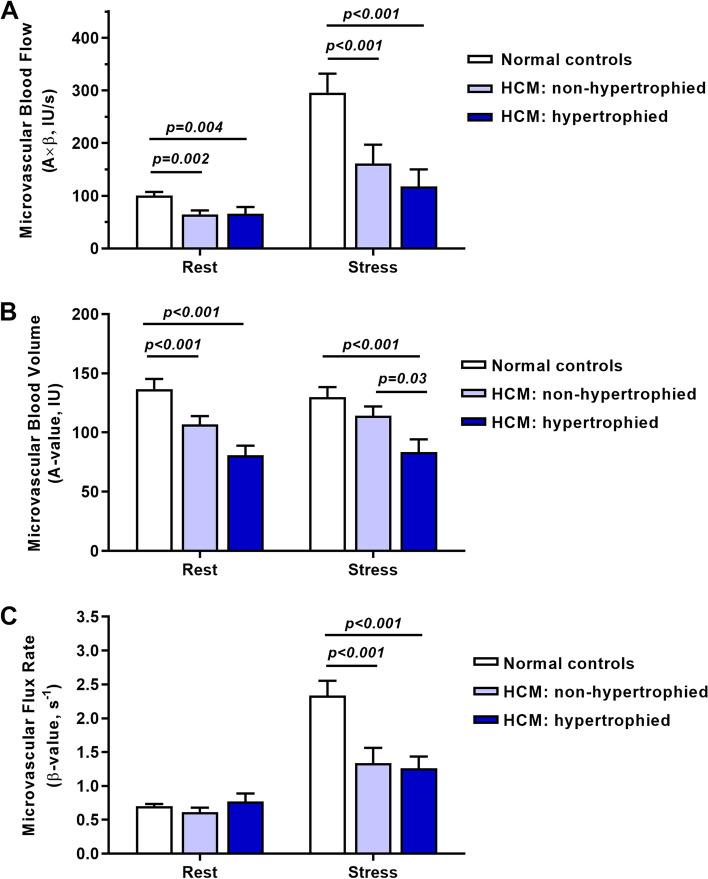
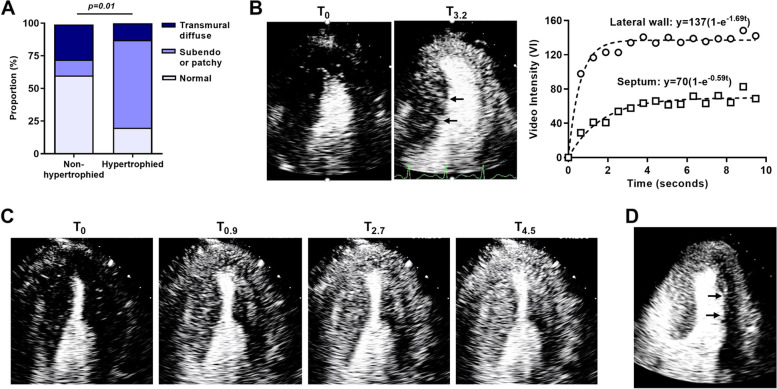
Methods: Regadenoson stress MCE was performed in patients with septal-variant HCM (n = 17) and healthy control subjects (n = 15). The presence and spatial distribution (transmural diffuse, patchy, subendocardial) of perfusion defects was determined by semiquantitative analysis. Kinetic analysis of time-intensity data was used to quantify MBF, microvascular flux rate (β), and microvascular blood volume. In patients undergoing septal myectomy (n = 3), MCE was repeated > 1 years after surgery. RESULTS: In HCM subjects, perfusion defects during stress occurred in the septum in 80%, and in non-hypertrophied regions in 40%. The majority of septal defects (83%) were patchy or subendocardial, while 67% of non-hypertrophied defects were transmural and diffuse. On quantitative analysis, hyperemic MBF was approximately 50% lower (p < 0.001) in the hypertrophied and non-hypertrophied regions of those with HCM compared to controls, largely based on an inability to augment β, although hypertrophic regions also had blood volume deficits. There was no correlation between hyperemic MBF and either percent fibrosis on magnetic resonance imaging or outflow gradient, yet those with higher degrees of fibrosis (≥ 5%) or severe gradients all had low septal MBF during regadenoson. Substantial improvement in hyperemic MBF was observed in two of the three subjects undergoing myectomy, both of whom had severe pre-surgical outflow gradients at rest.
Conclusion: Perfusion defects on vasodilator MCE are common in HCM, particularly in those with extensive fibrosis, but have a different spatial pattern for the hypertrophied and non-hypertrophied segments, likely reflecting different contributions of functional and structural abnormalities. Improvement in hyperemic perfusion is possible in those undergoing septal myectomy to relieve obstruction. TRIAL REGISTRATION: ClinicalTrials.gov NCT02560467.
期刊介绍:
Cardiovascular Ultrasound is an online journal, publishing peer-reviewed: original research; authoritative reviews; case reports on challenging and/or unusual diagnostic aspects; and expert opinions on new techniques and technologies. We are particularly interested in articles that include relevant images or video files, which provide an additional dimension to published articles and enhance understanding.
As an open access journal, Cardiovascular Ultrasound ensures high visibility for authors in addition to providing an up-to-date and freely available resource for the community. The journal welcomes discussion, and provides a forum for publishing opinion and debate ranging from biology to engineering to clinical echocardiography, with both speed and versatility.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
