Eliane Dohner, Marc von Tobel, Samuel Käser, René Fahrner
{"title":"由结肠假性梗阻引起的肠门、肠系膜及肾气性肠肺病。","authors":"Eliane Dohner, Marc von Tobel, Samuel Käser, René Fahrner","doi":"10.1515/iss-2021-0031","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Pneumatosis intestinalis is a rare condition with subserosal or submucosal gas-filled cysts of the gastrointestinal tract. It is often associated with acute mesenteric ischemia, but also non-ischemic causes are described.</p><p><strong>Case presentation: </strong>A 27-year-old male patient with severe congenital spastic tetraparesis presented to the emergency room with fever and reduced general condition. The patient was hypotonic and tachycardic, had a fever up to 39.7 °C and reduced peripheral oxygen saturation. The laboratory analyses revealed leukocytosis (16.7 G/L) and elevated CRP (162 mg/L).The patient was admitted to the intensive care unit (ICU) for invasive ventilator treatment because of global respiratory insufficiency and antibiotic therapy due to acute pneumonia and severe acute respiratory distress syndrome (ARDS). In addition, he suffered from colonic pseudo-obstruction but with persistent stool passage. After pulmonary recovery, he was transferred to the normal ward of internal medicine, but signs of colonic pseudo-obstruction were still present.Under therapy with diatrizoic acid and neostigmine, the abdomen was less distended, and the patient had regular bowel movements. After four days, the patient developed sudden acute abdominal pain and suffered sudden pulseless electrical activity. Immediate cardiopulmonary resuscitation was provided. After the return of spontaneous circulation, the patient underwent computed tomography (CT) and was re-admitted to the ICU. The CT scan showed massive dilatation of the colon, including pneumatosis coli, extensive gas formation within the mesenteric veins and arteries, including massive portal gas in the liver, the splenic vein, the renal veins, and disruption of abdominal aortic perfusion. The patient was then first presented for surgical evaluation, but due to futile prognosis, treatment was ceased on the ICU.</p><p><strong>Conclusions: </strong>In conclusion, colonic pseudo-obstruction might have led to colonic necrosis and consecutive massive gas formation within the mesenteric vessels. Therefore, intestinal passage should be restored as soon as possible to avoid possible mortality.</p>","PeriodicalId":44186,"journal":{"name":"Innovative Surgical Sciences","volume":"7 1","pages":"31-34"},"PeriodicalIF":1.2000,"publicationDate":"2022-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9352184/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pneumatosis intestinalis with portal, mesenteric and renal gas due to colonic pseudo-obstruction.\",\"authors\":\"Eliane Dohner, Marc von Tobel, Samuel Käser, René Fahrner\",\"doi\":\"10.1515/iss-2021-0031\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Pneumatosis intestinalis is a rare condition with subserosal or submucosal gas-filled cysts of the gastrointestinal tract. It is often associated with acute mesenteric ischemia, but also non-ischemic causes are described.</p><p><strong>Case presentation: </strong>A 27-year-old male patient with severe congenital spastic tetraparesis presented to the emergency room with fever and reduced general condition. The patient was hypotonic and tachycardic, had a fever up to 39.7 °C and reduced peripheral oxygen saturation. The laboratory analyses revealed leukocytosis (16.7 G/L) and elevated CRP (162 mg/L).The patient was admitted to the intensive care unit (ICU) for invasive ventilator treatment because of global respiratory insufficiency and antibiotic therapy due to acute pneumonia and severe acute respiratory distress syndrome (ARDS). In addition, he suffered from colonic pseudo-obstruction but with persistent stool passage. After pulmonary recovery, he was transferred to the normal ward of internal medicine, but signs of colonic pseudo-obstruction were still present.Under therapy with diatrizoic acid and neostigmine, the abdomen was less distended, and the patient had regular bowel movements. After four days, the patient developed sudden acute abdominal pain and suffered sudden pulseless electrical activity. Immediate cardiopulmonary resuscitation was provided. After the return of spontaneous circulation, the patient underwent computed tomography (CT) and was re-admitted to the ICU. The CT scan showed massive dilatation of the colon, including pneumatosis coli, extensive gas formation within the mesenteric veins and arteries, including massive portal gas in the liver, the splenic vein, the renal veins, and disruption of abdominal aortic perfusion. The patient was then first presented for surgical evaluation, but due to futile prognosis, treatment was ceased on the ICU.</p><p><strong>Conclusions: </strong>In conclusion, colonic pseudo-obstruction might have led to colonic necrosis and consecutive massive gas formation within the mesenteric vessels. Therefore, intestinal passage should be restored as soon as possible to avoid possible mortality.</p>\",\"PeriodicalId\":44186,\"journal\":{\"name\":\"Innovative Surgical Sciences\",\"volume\":\"7 1\",\"pages\":\"31-34\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2022-06-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9352184/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Innovative Surgical Sciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/iss-2021-0031\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Innovative Surgical Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/iss-2021-0031","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/3/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Pneumatosis intestinalis with portal, mesenteric and renal gas due to colonic pseudo-obstruction.
Objectives: Pneumatosis intestinalis is a rare condition with subserosal or submucosal gas-filled cysts of the gastrointestinal tract. It is often associated with acute mesenteric ischemia, but also non-ischemic causes are described.
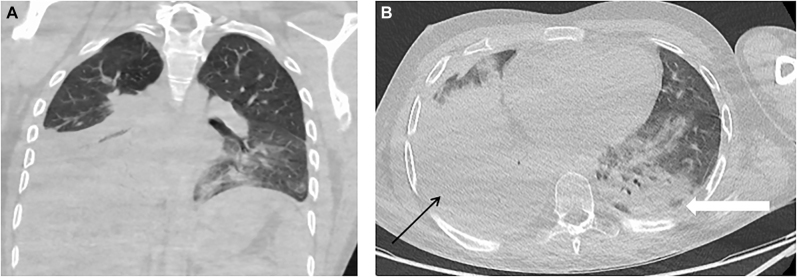
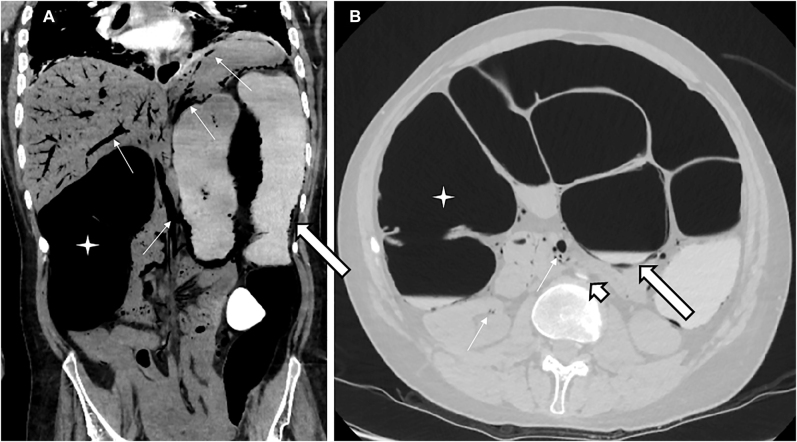
Case presentation: A 27-year-old male patient with severe congenital spastic tetraparesis presented to the emergency room with fever and reduced general condition. The patient was hypotonic and tachycardic, had a fever up to 39.7 °C and reduced peripheral oxygen saturation. The laboratory analyses revealed leukocytosis (16.7 G/L) and elevated CRP (162 mg/L).The patient was admitted to the intensive care unit (ICU) for invasive ventilator treatment because of global respiratory insufficiency and antibiotic therapy due to acute pneumonia and severe acute respiratory distress syndrome (ARDS). In addition, he suffered from colonic pseudo-obstruction but with persistent stool passage. After pulmonary recovery, he was transferred to the normal ward of internal medicine, but signs of colonic pseudo-obstruction were still present.Under therapy with diatrizoic acid and neostigmine, the abdomen was less distended, and the patient had regular bowel movements. After four days, the patient developed sudden acute abdominal pain and suffered sudden pulseless electrical activity. Immediate cardiopulmonary resuscitation was provided. After the return of spontaneous circulation, the patient underwent computed tomography (CT) and was re-admitted to the ICU. The CT scan showed massive dilatation of the colon, including pneumatosis coli, extensive gas formation within the mesenteric veins and arteries, including massive portal gas in the liver, the splenic vein, the renal veins, and disruption of abdominal aortic perfusion. The patient was then first presented for surgical evaluation, but due to futile prognosis, treatment was ceased on the ICU.
Conclusions: In conclusion, colonic pseudo-obstruction might have led to colonic necrosis and consecutive massive gas formation within the mesenteric vessels. Therefore, intestinal passage should be restored as soon as possible to avoid possible mortality.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
