Wenjun Li, Edward J Stanek, Elizabeth R Bertone-Johnson
{"title":"在流行率估计中应该使用协变量调整吗?","authors":"Wenjun Li, Edward J Stanek, Elizabeth R Bertone-Johnson","doi":"10.1186/1742-5573-5-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adjustment for covariates (also called auxiliary variables in survey sampling literature) is commonly applied in health surveys to reduce the variances of the prevalence estimators. In theory, adjusted prevalence estimators are more accurate when variance components are known. In practice, variance components needed to achieve the adjustment are unknown and their sample estimators are used instead. The uncertainty introduced by estimating variance components may overshadow the reduction in the variance of the prevalence estimators due to adjustment. We present empirical guidelines indicating when adjusted prevalence estimators should be considered, using gender adjusted and unadjusted smoking prevalence as an illustration.</p><p><strong>Methods: </strong>We compare the accuracy of adjusted and unadjusted prevalence estimators via simulation. We simulate simple random samples from hypothetical populations with the proportion of males ranging from 30% to 70%, the smoking prevalence ranging from 15% to 35%, and the ratio of male to female smoking prevalence ranging from 1 to 4. The ranges of gender proportions and smoking prevalences reflect the conditions in 1999-2003 Behavioral Risk Factors Surveillance System (BRFSS) data for Massachusetts. From each population, 10,000 samples are selected and the ratios of the variance of the adjusted prevalence estimators to the variance of the unadjusted (crude) ones are computed and plotted against the proportion of males by population prevalence, as well as by population and sample sizes. The prevalence ratio thresholds, above which adjusted prevalence estimators have smaller variances, are determined graphically.</p><p><strong>Results: </strong>In many practical settings, gender adjustment results in less accuracy. Whether or not there is better accuracy with adjustment depends on sample sizes, gender proportions and ratios between male and female prevalences. In populations with equal number of males and females and smoking prevalence of 20%, the adjusted prevalence estimators are more accurate when the ratios of male to female prevalences are above 2.4, 1.8, 1.6, 1.4 and 1.3 for sample sizes of 25, 50, 100, 150 and 200, respectively.</p><p><strong>Conclusion: </strong>Adjustment for covariates will not result in more accurate prevalence estimator when ratio of male to female prevalences is close to one, sample size is small and risk factor prevalence is low. For example, when reporting smoking prevalence based on simple random sampling, gender adjustment is recommended only when sample size is greater than 200.</p>","PeriodicalId":87082,"journal":{"name":"Epidemiologic perspectives & innovations : EP+I","volume":" ","pages":"2"},"PeriodicalIF":0.0000,"publicationDate":"2008-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1742-5573-5-2","citationCount":"2","resultStr":"{\"title\":\"Should adjustment for covariates be used in prevalence estimations?\",\"authors\":\"Wenjun Li, Edward J Stanek, Elizabeth R Bertone-Johnson\",\"doi\":\"10.1186/1742-5573-5-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Adjustment for covariates (also called auxiliary variables in survey sampling literature) is commonly applied in health surveys to reduce the variances of the prevalence estimators. In theory, adjusted prevalence estimators are more accurate when variance components are known. In practice, variance components needed to achieve the adjustment are unknown and their sample estimators are used instead. The uncertainty introduced by estimating variance components may overshadow the reduction in the variance of the prevalence estimators due to adjustment. We present empirical guidelines indicating when adjusted prevalence estimators should be considered, using gender adjusted and unadjusted smoking prevalence as an illustration.</p><p><strong>Methods: </strong>We compare the accuracy of adjusted and unadjusted prevalence estimators via simulation. We simulate simple random samples from hypothetical populations with the proportion of males ranging from 30% to 70%, the smoking prevalence ranging from 15% to 35%, and the ratio of male to female smoking prevalence ranging from 1 to 4. The ranges of gender proportions and smoking prevalences reflect the conditions in 1999-2003 Behavioral Risk Factors Surveillance System (BRFSS) data for Massachusetts. From each population, 10,000 samples are selected and the ratios of the variance of the adjusted prevalence estimators to the variance of the unadjusted (crude) ones are computed and plotted against the proportion of males by population prevalence, as well as by population and sample sizes. The prevalence ratio thresholds, above which adjusted prevalence estimators have smaller variances, are determined graphically.</p><p><strong>Results: </strong>In many practical settings, gender adjustment results in less accuracy. Whether or not there is better accuracy with adjustment depends on sample sizes, gender proportions and ratios between male and female prevalences. In populations with equal number of males and females and smoking prevalence of 20%, the adjusted prevalence estimators are more accurate when the ratios of male to female prevalences are above 2.4, 1.8, 1.6, 1.4 and 1.3 for sample sizes of 25, 50, 100, 150 and 200, respectively.</p><p><strong>Conclusion: </strong>Adjustment for covariates will not result in more accurate prevalence estimator when ratio of male to female prevalences is close to one, sample size is small and risk factor prevalence is low. For example, when reporting smoking prevalence based on simple random sampling, gender adjustment is recommended only when sample size is greater than 200.</p>\",\"PeriodicalId\":87082,\"journal\":{\"name\":\"Epidemiologic perspectives & innovations : EP+I\",\"volume\":\" \",\"pages\":\"2\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2008-01-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/1742-5573-5-2\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Epidemiologic perspectives & innovations : EP+I\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/1742-5573-5-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epidemiologic perspectives & innovations : EP+I","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1742-5573-5-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Should adjustment for covariates be used in prevalence estimations?
Background: Adjustment for covariates (also called auxiliary variables in survey sampling literature) is commonly applied in health surveys to reduce the variances of the prevalence estimators. In theory, adjusted prevalence estimators are more accurate when variance components are known. In practice, variance components needed to achieve the adjustment are unknown and their sample estimators are used instead. The uncertainty introduced by estimating variance components may overshadow the reduction in the variance of the prevalence estimators due to adjustment. We present empirical guidelines indicating when adjusted prevalence estimators should be considered, using gender adjusted and unadjusted smoking prevalence as an illustration.
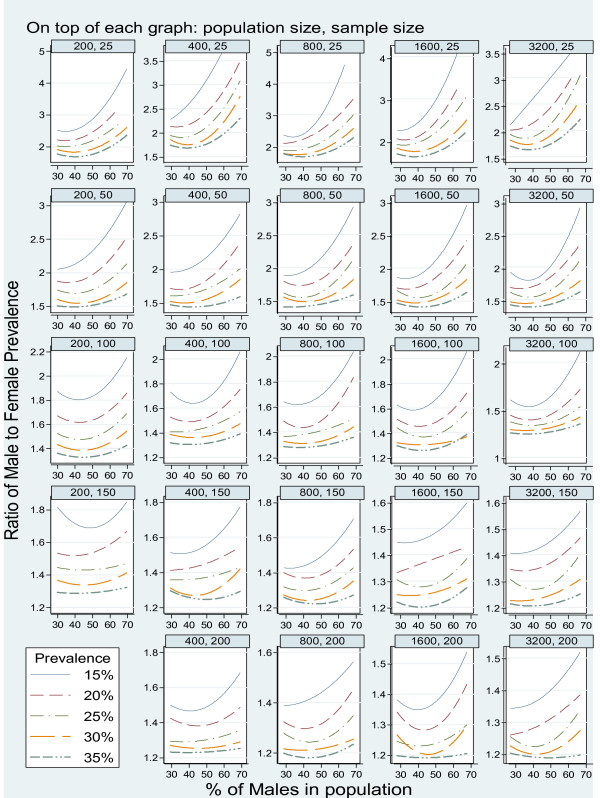
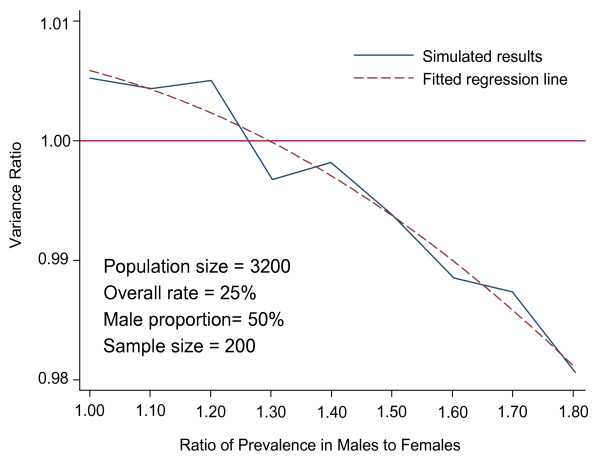
Methods: We compare the accuracy of adjusted and unadjusted prevalence estimators via simulation. We simulate simple random samples from hypothetical populations with the proportion of males ranging from 30% to 70%, the smoking prevalence ranging from 15% to 35%, and the ratio of male to female smoking prevalence ranging from 1 to 4. The ranges of gender proportions and smoking prevalences reflect the conditions in 1999-2003 Behavioral Risk Factors Surveillance System (BRFSS) data for Massachusetts. From each population, 10,000 samples are selected and the ratios of the variance of the adjusted prevalence estimators to the variance of the unadjusted (crude) ones are computed and plotted against the proportion of males by population prevalence, as well as by population and sample sizes. The prevalence ratio thresholds, above which adjusted prevalence estimators have smaller variances, are determined graphically.
Results: In many practical settings, gender adjustment results in less accuracy. Whether or not there is better accuracy with adjustment depends on sample sizes, gender proportions and ratios between male and female prevalences. In populations with equal number of males and females and smoking prevalence of 20%, the adjusted prevalence estimators are more accurate when the ratios of male to female prevalences are above 2.4, 1.8, 1.6, 1.4 and 1.3 for sample sizes of 25, 50, 100, 150 and 200, respectively.
Conclusion: Adjustment for covariates will not result in more accurate prevalence estimator when ratio of male to female prevalences is close to one, sample size is small and risk factor prevalence is low. For example, when reporting smoking prevalence based on simple random sampling, gender adjustment is recommended only when sample size is greater than 200.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
