Justin Johannesen, Rena Fukuda, David T Zhang, Katherine Tak, Rachel Meier, Hannah Agoglia, Evelyn Horn, Richard B Devereux, Jonathan W Weinsaft, Jiwon Kim
{"title":"超声心动图斑点跟踪和心脏磁共振特征跟踪量化右心室应变的直接比较:功能性二尖瓣反流的前瞻性多模态研究。","authors":"Justin Johannesen, Rena Fukuda, David T Zhang, Katherine Tak, Rachel Meier, Hannah Agoglia, Evelyn Horn, Richard B Devereux, Jonathan W Weinsaft, Jiwon Kim","doi":"10.1186/s44156-022-00011-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Functional mitral regurgitation (FMR) is a known risk factor for right ventricular dysfunction (RV<sub>DYS</sub>). RV global longitudinal strain (GLS) is an emerging index of RV function; however, the magnitude of agreement between RV GLS by echocardiography (echo) and cardiac magnetic resonance (CMR) and the relative utility of each modality for both the diagnosis of RV<sub>DYS</sub> and prognostication of all-cause mortality and heart failure hospitalization remain unknown.</p><p><strong>Results: </strong>32% of patients had RV<sub>DYS</sub> (EF < 50%) on CMR, among whom there was more advanced NYHA class and lower LV and RV ejection fraction (all p < 0.05). RV GLS was impaired in patients with RV<sub>DYS</sub> whether quantified via STE or FT-CMR, with strong correlation between modalities (r = 0.81). Both STE and FT-CMR derived GLS yielded excellent detection of RV<sub>DYS</sub> (AUC 0.94 for both), paralleling similar performance for free wall strain by both modalities (FT-CMR AUC 0.94, STE AUC 0.92) with lower accuracy demonstrated by STE derived septal strain (STE AUC 0.78 and FT-CMR AUC 0.92). RV S' and TAPSE showed lower diagnostic accuracy (RV S' AUC 0.77 and TAPSE AUC 0.81). During median follow up of 51 months (IQR 42, 60 months), all-cause mortality or HF hospitalization occurred in 25% (n = 25). Both STE and FT-CMR derived RV GLS stratified risk for adverse prognosis (STE p = 0.007, FT-CMR p = 0.005) whereas conventional RV indices, TAPSE and RV S', did not (TAPSE p = 0.30, S' p = 0.69).</p><p><strong>Conclusion: </strong>RV GLS is a robust marker of RV<sub>DYS</sub> irrespective of modality which provides incremental diagnostic value and improves risk stratification for event free survival beyond conventional RV indices.</p>","PeriodicalId":45749,"journal":{"name":"Echo Research and Practice","volume":" ","pages":"11"},"PeriodicalIF":2.4000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9623949/pdf/","citationCount":"0","resultStr":"{\"title\":\"Direct comparison of echocardiography speckle tracking and cardiac magnetic resonance feature tracking for quantification of right ventricular strain: a prospective intermodality study in functional mitral regurgitation.\",\"authors\":\"Justin Johannesen, Rena Fukuda, David T Zhang, Katherine Tak, Rachel Meier, Hannah Agoglia, Evelyn Horn, Richard B Devereux, Jonathan W Weinsaft, Jiwon Kim\",\"doi\":\"10.1186/s44156-022-00011-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Functional mitral regurgitation (FMR) is a known risk factor for right ventricular dysfunction (RV<sub>DYS</sub>). RV global longitudinal strain (GLS) is an emerging index of RV function; however, the magnitude of agreement between RV GLS by echocardiography (echo) and cardiac magnetic resonance (CMR) and the relative utility of each modality for both the diagnosis of RV<sub>DYS</sub> and prognostication of all-cause mortality and heart failure hospitalization remain unknown.</p><p><strong>Results: </strong>32% of patients had RV<sub>DYS</sub> (EF < 50%) on CMR, among whom there was more advanced NYHA class and lower LV and RV ejection fraction (all p < 0.05). RV GLS was impaired in patients with RV<sub>DYS</sub> whether quantified via STE or FT-CMR, with strong correlation between modalities (r = 0.81). Both STE and FT-CMR derived GLS yielded excellent detection of RV<sub>DYS</sub> (AUC 0.94 for both), paralleling similar performance for free wall strain by both modalities (FT-CMR AUC 0.94, STE AUC 0.92) with lower accuracy demonstrated by STE derived septal strain (STE AUC 0.78 and FT-CMR AUC 0.92). RV S' and TAPSE showed lower diagnostic accuracy (RV S' AUC 0.77 and TAPSE AUC 0.81). During median follow up of 51 months (IQR 42, 60 months), all-cause mortality or HF hospitalization occurred in 25% (n = 25). Both STE and FT-CMR derived RV GLS stratified risk for adverse prognosis (STE p = 0.007, FT-CMR p = 0.005) whereas conventional RV indices, TAPSE and RV S', did not (TAPSE p = 0.30, S' p = 0.69).</p><p><strong>Conclusion: </strong>RV GLS is a robust marker of RV<sub>DYS</sub> irrespective of modality which provides incremental diagnostic value and improves risk stratification for event free survival beyond conventional RV indices.</p>\",\"PeriodicalId\":45749,\"journal\":{\"name\":\"Echo Research and Practice\",\"volume\":\" \",\"pages\":\"11\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2022-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9623949/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Echo Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44156-022-00011-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Echo Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44156-022-00011-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:功能性二尖瓣反流(FMR)是右室功能障碍(RVDYS)的已知危险因素。RV全局纵向应变(GLS)是RV函数的一个新兴指标;然而,超声心动图(echo)和心脏磁共振(CMR)的RV GLS之间的一致性程度以及每种模式在诊断RVDYS和预测全因死亡率和心力衰竭住院治疗方面的相对效用仍然未知。结果:32%的患者有RVDYS (EF DYS),无论是通过STE还是FT-CMR量化,两种方式之间有很强的相关性(r = 0.81)。STE和FT-CMR衍生的GLS都能很好地检测RVDYS(两者的AUC均为0.94),两种方法对自由壁应变的检测效果相似(FT-CMR的AUC为0.94,STE的AUC为0.92),STE衍生的间隔应变的准确度较低(STE的AUC为0.78,FT-CMR的AUC为0.92)。RV S'和TAPSE的诊断准确率较低(RV S' AUC为0.77,TAPSE AUC为0.81)。中位随访51个月(IQR为42个月,60个月),全因死亡率或HF住院率为25% (n = 25)。STE和FT-CMR均可得出RV GLS分层不良预后风险(STE p = 0.007, FT-CMR p = 0.005),而传统的RV指标TAPSE和RV S′则不能(TAPSE p = 0.30, S′p = 0.69)。结论:与常规RV指标相比,RVDYS GLS是RVDYS的一个强有力的标志物,提供了增量诊断价值,并改善了无事件生存的风险分层。
Direct comparison of echocardiography speckle tracking and cardiac magnetic resonance feature tracking for quantification of right ventricular strain: a prospective intermodality study in functional mitral regurgitation.
Background: Functional mitral regurgitation (FMR) is a known risk factor for right ventricular dysfunction (RVDYS). RV global longitudinal strain (GLS) is an emerging index of RV function; however, the magnitude of agreement between RV GLS by echocardiography (echo) and cardiac magnetic resonance (CMR) and the relative utility of each modality for both the diagnosis of RVDYS and prognostication of all-cause mortality and heart failure hospitalization remain unknown.
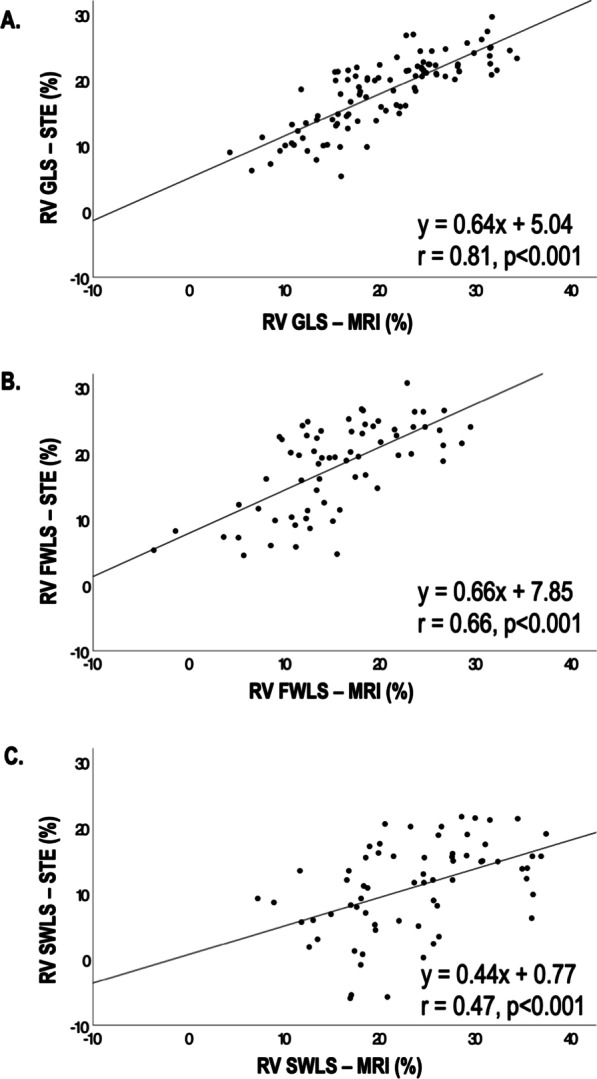
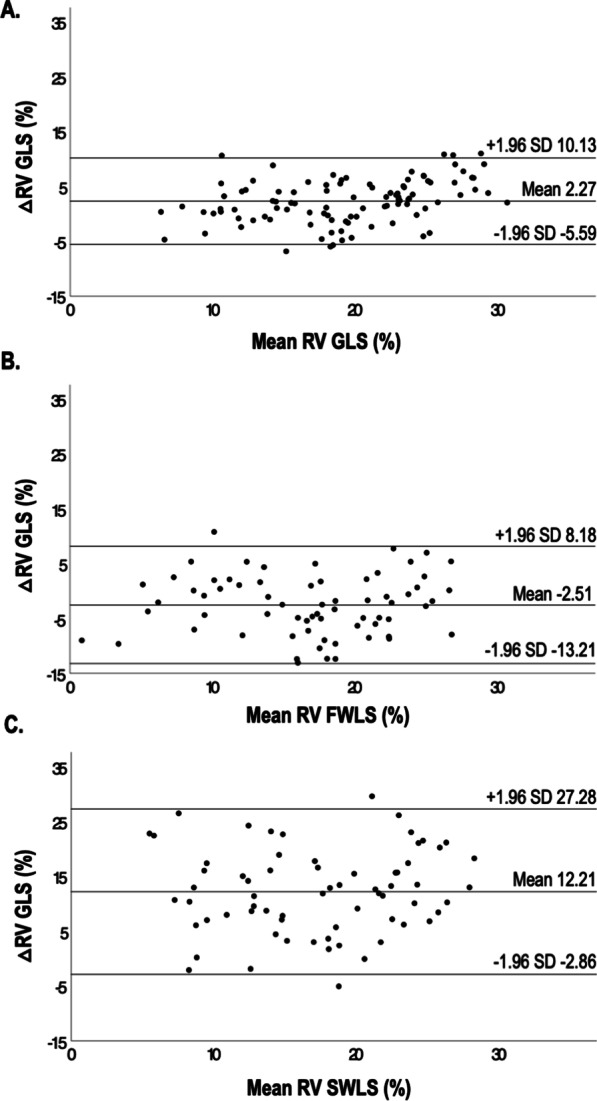
Results: 32% of patients had RVDYS (EF < 50%) on CMR, among whom there was more advanced NYHA class and lower LV and RV ejection fraction (all p < 0.05). RV GLS was impaired in patients with RVDYS whether quantified via STE or FT-CMR, with strong correlation between modalities (r = 0.81). Both STE and FT-CMR derived GLS yielded excellent detection of RVDYS (AUC 0.94 for both), paralleling similar performance for free wall strain by both modalities (FT-CMR AUC 0.94, STE AUC 0.92) with lower accuracy demonstrated by STE derived septal strain (STE AUC 0.78 and FT-CMR AUC 0.92). RV S' and TAPSE showed lower diagnostic accuracy (RV S' AUC 0.77 and TAPSE AUC 0.81). During median follow up of 51 months (IQR 42, 60 months), all-cause mortality or HF hospitalization occurred in 25% (n = 25). Both STE and FT-CMR derived RV GLS stratified risk for adverse prognosis (STE p = 0.007, FT-CMR p = 0.005) whereas conventional RV indices, TAPSE and RV S', did not (TAPSE p = 0.30, S' p = 0.69).
Conclusion: RV GLS is a robust marker of RVDYS irrespective of modality which provides incremental diagnostic value and improves risk stratification for event free survival beyond conventional RV indices.
期刊介绍:
Echo Research and Practice aims to be the premier international journal for physicians, sonographers, nurses and other allied health professionals practising echocardiography and other cardiac imaging modalities. This open-access journal publishes quality clinical and basic research, reviews, videos, education materials and selected high-interest case reports and videos across all echocardiography modalities and disciplines, including paediatrics, anaesthetics, general practice, acute medicine and intensive care. Multi-modality studies primarily featuring the use of cardiac ultrasound in clinical practice, in association with Cardiac Computed Tomography, Cardiovascular Magnetic Resonance or Nuclear Cardiology are of interest. Topics include, but are not limited to: 2D echocardiography 3D echocardiography Comparative imaging techniques – CCT, CMR and Nuclear Cardiology Congenital heart disease, including foetal echocardiography Contrast echocardiography Critical care echocardiography Deformation imaging Doppler echocardiography Interventional echocardiography Intracardiac echocardiography Intraoperative echocardiography Prosthetic valves Stress echocardiography Technical innovations Transoesophageal echocardiography Valve disease.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
