Seyeon Park, Sang-Wook Shin, Hye-Jin Kim, Gyeong-Jo Byeon, Ji-Uk Yoon, Eun-Jung Kim, Hee Young Kim
{"title":"为儿科患者选择正确尺寸的气管插管。","authors":"Seyeon Park, Sang-Wook Shin, Hye-Jin Kim, Gyeong-Jo Byeon, Ji-Uk Yoon, Eun-Jung Kim, Hee Young Kim","doi":"10.17085/apm.22215","DOIUrl":null,"url":null,"abstract":"<p><p>Selection and insertion of an endotracheal tube (ETT) of appropriate size for airway management during general anesthesia in pediatric patients is very important. A very small ETT increases the risk of inadequate ventilation, air leakage, and aspiration, whereas a very large ETT may cause serious complications including airway damage, post-intubation croup, and, in severe cases, subglottic stenosis. Although the pediatric larynx is conical, the narrowest part, the rima glottidis, is cylindrical in the anteroposterior dimension, regardless of development, and the cricoid ring is slightly elliptical. A cuffed ETT reduces the number of endotracheal intubation attempts, and if cuff pressure can be maintained within a safe range, the risk of airway damage may not be greater than that of an ETT without cuff. The age-based formula suggested by Cole (age/4 + 4) has long been used to select the appropriate ETT size in children. Because age-based formulas in children are not always accurate, various alternative methods for estimating the ETT size have been examined and suggested. Chest radiography, ultrasound, and a three-dimensional airway model can be used to determine the appropriate ETT size; however, there are several limitations.</p>","PeriodicalId":7801,"journal":{"name":"Anesthesia and pain medicine","volume":" ","pages":"352-360"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/31/3c/apm-22215.PMC9663958.pdf","citationCount":"0","resultStr":"{\"title\":\"Choice of the correct size of endotracheal tube in pediatric patients.\",\"authors\":\"Seyeon Park, Sang-Wook Shin, Hye-Jin Kim, Gyeong-Jo Byeon, Ji-Uk Yoon, Eun-Jung Kim, Hee Young Kim\",\"doi\":\"10.17085/apm.22215\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Selection and insertion of an endotracheal tube (ETT) of appropriate size for airway management during general anesthesia in pediatric patients is very important. A very small ETT increases the risk of inadequate ventilation, air leakage, and aspiration, whereas a very large ETT may cause serious complications including airway damage, post-intubation croup, and, in severe cases, subglottic stenosis. Although the pediatric larynx is conical, the narrowest part, the rima glottidis, is cylindrical in the anteroposterior dimension, regardless of development, and the cricoid ring is slightly elliptical. A cuffed ETT reduces the number of endotracheal intubation attempts, and if cuff pressure can be maintained within a safe range, the risk of airway damage may not be greater than that of an ETT without cuff. The age-based formula suggested by Cole (age/4 + 4) has long been used to select the appropriate ETT size in children. Because age-based formulas in children are not always accurate, various alternative methods for estimating the ETT size have been examined and suggested. Chest radiography, ultrasound, and a three-dimensional airway model can be used to determine the appropriate ETT size; however, there are several limitations.</p>\",\"PeriodicalId\":7801,\"journal\":{\"name\":\"Anesthesia and pain medicine\",\"volume\":\" \",\"pages\":\"352-360\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/31/3c/apm-22215.PMC9663958.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anesthesia and pain medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17085/apm.22215\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.22215","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
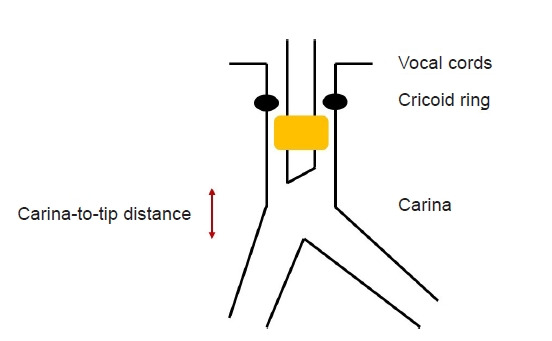
在对儿科患者进行全身麻醉时,选择和插入大小合适的气管导管(ETT)以进行气道管理非常重要。过小的 ETT 会增加通气不足、漏气和吸入的风险,而过大的 ETT 则可能导致严重的并发症,包括气道损伤、插管后气管痉挛,严重时还会导致声门下狭窄。虽然小儿喉部呈圆锥形,但其最狭窄的部分(声门区)在前后维度上呈圆柱形,与发育情况无关,环甲膜环则略呈椭圆形。带充气罩囊的 ETT 可减少气管插管的次数,如果充气罩囊压力能保持在安全范围内,气道损伤的风险可能并不比不带充气罩囊的 ETT 大。长期以来,Cole 提出的基于年龄的公式(年龄/4 + 4)一直被用于为儿童选择合适的 ETT 大小。由于以儿童年龄为基础的公式并不总是准确的,因此人们研究并提出了各种估算 ETT 大小的替代方法。胸片、超声波和三维气道模型可用于确定合适的 ETT 大小;但这些方法都有一些局限性。
Choice of the correct size of endotracheal tube in pediatric patients.
Selection and insertion of an endotracheal tube (ETT) of appropriate size for airway management during general anesthesia in pediatric patients is very important. A very small ETT increases the risk of inadequate ventilation, air leakage, and aspiration, whereas a very large ETT may cause serious complications including airway damage, post-intubation croup, and, in severe cases, subglottic stenosis. Although the pediatric larynx is conical, the narrowest part, the rima glottidis, is cylindrical in the anteroposterior dimension, regardless of development, and the cricoid ring is slightly elliptical. A cuffed ETT reduces the number of endotracheal intubation attempts, and if cuff pressure can be maintained within a safe range, the risk of airway damage may not be greater than that of an ETT without cuff. The age-based formula suggested by Cole (age/4 + 4) has long been used to select the appropriate ETT size in children. Because age-based formulas in children are not always accurate, various alternative methods for estimating the ETT size have been examined and suggested. Chest radiography, ultrasound, and a three-dimensional airway model can be used to determine the appropriate ETT size; however, there are several limitations.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
