Hye-Mee Kwon, Jae Hwan Kim, Ji-Young Kim, Gyu-Sam Hwang
{"title":"危重肝移植合并冠心病患者5年全因死亡率:急性-慢性肝衰竭分析","authors":"Hye-Mee Kwon, Jae Hwan Kim, Ji-Young Kim, Gyu-Sam Hwang","doi":"10.17085/apm.22168","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with acute-on-chronic liver failure (ACLF) are critically ill and have high waiting-list mortality. Although studies demonstrated that appropriately treated coronary artery disease (CAD) should not be regarded as a contraindication to liver transplant (LT), data regarding long-term outcomes in critically ill liver LT recipients are lacking. The aim of this study was to compare the rates of all-cause death at 5 years following LT in patients with ACLF with or without CAD.</p><p><strong>Methods: </strong>Between 2010 and 2020, we evaluated 921 consecutive LT patients (MELD score, 32 ± 9) and ACLF classified by CLIF-C ACLF score. Up to 5-year all-cause death according to the CAD status was examined. CAD was defined as a preoperative history of coronary artery bypass graft or a percutaneous intervention and old myocardial infarction. Kaplan-Meier survival analysis was used.</p><p><strong>Results: </strong>Up to 5 years, 212 (23.0%) of all ACLF patients (n = 921) in whom 17 (29.3%) of 58 CAD patients died. In patients with CAD (6.3%, 58/921), the Kaplan-Meier cumulative mortality rate at 5 years was numerically higher but was not statistically significant when compared with those without CAD (32.9% vs. 23.5%, log-rank, P = 0.25). In subgr oup analysis, there were comparable risks of cumulative mortalities at 5 years across the stratification of ACLF grade 1, 2, and 3 (log-rank P = 0.062, P = 0.72, and P = 0.999, respectively).</p><p><strong>Conclusions: </strong>All-cause mortality is high in patients with ACLF after LT but is not related to the presence of revascularized or treated CAD, across the stratification of ACLF grades.</p>","PeriodicalId":7801,"journal":{"name":"Anesthesia and pain medicine","volume":" ","pages":"412-419"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/31/apm-22168.PMC9663955.pdf","citationCount":"1","resultStr":"{\"title\":\"Five-year all-cause mortality in critically ill liver transplant patients with coronary artery disease: analysis of acute-on chronic liver failure.\",\"authors\":\"Hye-Mee Kwon, Jae Hwan Kim, Ji-Young Kim, Gyu-Sam Hwang\",\"doi\":\"10.17085/apm.22168\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with acute-on-chronic liver failure (ACLF) are critically ill and have high waiting-list mortality. Although studies demonstrated that appropriately treated coronary artery disease (CAD) should not be regarded as a contraindication to liver transplant (LT), data regarding long-term outcomes in critically ill liver LT recipients are lacking. The aim of this study was to compare the rates of all-cause death at 5 years following LT in patients with ACLF with or without CAD.</p><p><strong>Methods: </strong>Between 2010 and 2020, we evaluated 921 consecutive LT patients (MELD score, 32 ± 9) and ACLF classified by CLIF-C ACLF score. Up to 5-year all-cause death according to the CAD status was examined. CAD was defined as a preoperative history of coronary artery bypass graft or a percutaneous intervention and old myocardial infarction. Kaplan-Meier survival analysis was used.</p><p><strong>Results: </strong>Up to 5 years, 212 (23.0%) of all ACLF patients (n = 921) in whom 17 (29.3%) of 58 CAD patients died. In patients with CAD (6.3%, 58/921), the Kaplan-Meier cumulative mortality rate at 5 years was numerically higher but was not statistically significant when compared with those without CAD (32.9% vs. 23.5%, log-rank, P = 0.25). In subgr oup analysis, there were comparable risks of cumulative mortalities at 5 years across the stratification of ACLF grade 1, 2, and 3 (log-rank P = 0.062, P = 0.72, and P = 0.999, respectively).</p><p><strong>Conclusions: </strong>All-cause mortality is high in patients with ACLF after LT but is not related to the presence of revascularized or treated CAD, across the stratification of ACLF grades.</p>\",\"PeriodicalId\":7801,\"journal\":{\"name\":\"Anesthesia and pain medicine\",\"volume\":\" \",\"pages\":\"412-419\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/31/apm-22168.PMC9663955.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anesthesia and pain medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17085/apm.22168\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.22168","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
背景:急性伴慢性肝衰竭(ACLF)患者病情危重,等待名单死亡率高。尽管研究表明,适当治疗的冠状动脉疾病(CAD)不应被视为肝移植(LT)的禁忌症,但关于危重肝移植受体的长期预后的数据缺乏。本研究的目的是比较合并或不合并CAD的ACLF患者LT后5年的全因死亡率。方法:2010年至2020年,我们对921例连续LT患者(MELD评分,32±9)和CLIF-C ACLF评分分级的ACLF进行了评估。根据CAD状态检查了长达5年的全因死亡。CAD定义为术前冠状动脉搭桥术或经皮介入治疗史和陈旧性心肌梗死史。采用Kaplan-Meier生存分析。结果:5年内,所有ACLF患者(n = 921)中有212例(23.0%)死亡,其中58例CAD患者中有17例(29.3%)死亡。在CAD患者中(6.3%,58/921),5年Kaplan-Meier累积死亡率在数值上高于非CAD患者(32.9% vs. 23.5%, log-rank, P = 0.25)。在亚组分析中,ACLF 1级、2级和3级分层中,5年累积死亡风险可比较(log-rank分别为P = 0.062、P = 0.72和P = 0.999)。结论:肝移植后ACLF患者的全因死亡率很高,但与存在血运重建或治疗的CAD无关,跨ACLF等级分层。
Five-year all-cause mortality in critically ill liver transplant patients with coronary artery disease: analysis of acute-on chronic liver failure.
Background: Patients with acute-on-chronic liver failure (ACLF) are critically ill and have high waiting-list mortality. Although studies demonstrated that appropriately treated coronary artery disease (CAD) should not be regarded as a contraindication to liver transplant (LT), data regarding long-term outcomes in critically ill liver LT recipients are lacking. The aim of this study was to compare the rates of all-cause death at 5 years following LT in patients with ACLF with or without CAD.
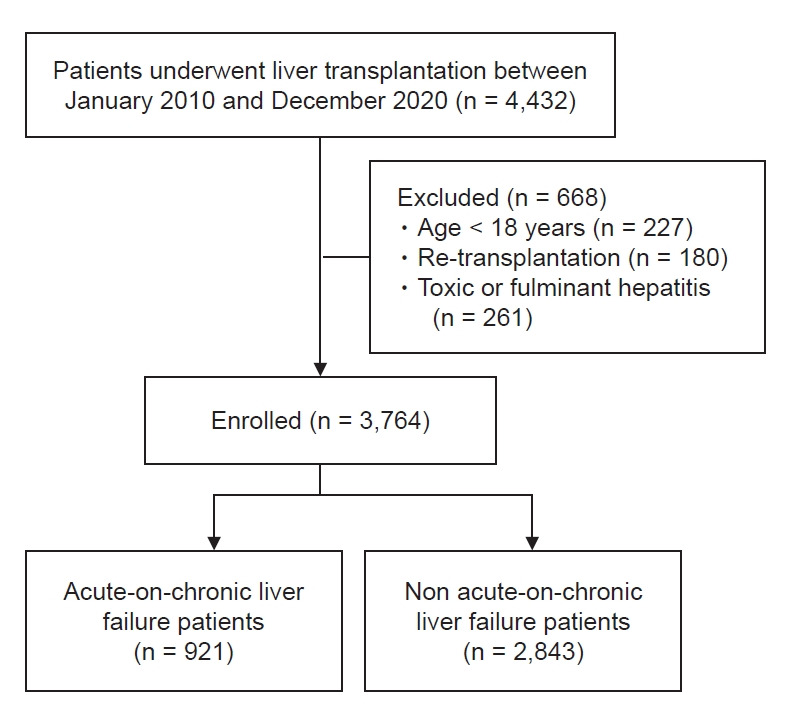
Methods: Between 2010 and 2020, we evaluated 921 consecutive LT patients (MELD score, 32 ± 9) and ACLF classified by CLIF-C ACLF score. Up to 5-year all-cause death according to the CAD status was examined. CAD was defined as a preoperative history of coronary artery bypass graft or a percutaneous intervention and old myocardial infarction. Kaplan-Meier survival analysis was used.
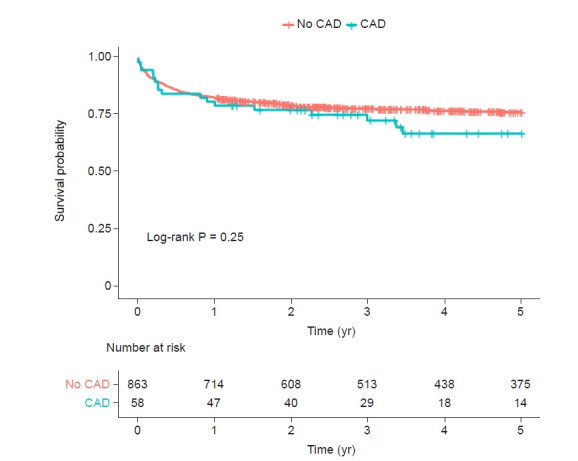
Results: Up to 5 years, 212 (23.0%) of all ACLF patients (n = 921) in whom 17 (29.3%) of 58 CAD patients died. In patients with CAD (6.3%, 58/921), the Kaplan-Meier cumulative mortality rate at 5 years was numerically higher but was not statistically significant when compared with those without CAD (32.9% vs. 23.5%, log-rank, P = 0.25). In subgr oup analysis, there were comparable risks of cumulative mortalities at 5 years across the stratification of ACLF grade 1, 2, and 3 (log-rank P = 0.062, P = 0.72, and P = 0.999, respectively).
Conclusions: All-cause mortality is high in patients with ACLF after LT but is not related to the presence of revascularized or treated CAD, across the stratification of ACLF grades.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
