{"title":"IGH/BCL2状态比组织学分级和其他分子标记更能预测原发性脾滤泡性淋巴瘤的临床病理行为。","authors":"Cherian Verghese, Weihong Li, Nanuli Gvazava, Emmanouil Alimpertis, Navkirat Kahlon, Hongliu Sun, Robert Booth","doi":"10.1177/2632010X221129242","DOIUrl":null,"url":null,"abstract":"<p><p>Splenic lymphoma may be primary or secondary. Primary splenic lymphoma's are rare and usually of follicular cell origin representing <1% of Non-Hodgkin's Lymphoma's. Most are secondary with 35% representing Marginal Cell sub-type with the rest being Diffuse Large B-Cell Lymphoma's. Unlike the uniformly aggressive clinical course of Diffuse Large B-Cell Lymphoma's, biological behavior of Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma remains less well defined. We present here a solitary splenic mass confirmed as Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma after a diagnostic splenectomy. Biopsy revealed monomorphic small lymphoid cells with low grade mitotic activity. Flow cytometry showed a lambda restricted population of B-Cells displaying dim CD19 and CD10. The cells were negative for CD5, CD11c, and CD103. FISH was negative for IGH/BCL2 fusion unlike nodal Follicular Lymphoma's which are usually positive for this translocation. Evidence from this case and a review of literature support the finding that Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma is less likely to have the classic IGH-BCL2 fusion and the associated chromosomal 14;18 translocation. This profile is associated with less aggressive clinical behavior even when histopathology represents a high-grade pattern. In such cases splenectomy alone is adequate for localized disease when negative for IGH/BCL2 fusion regardless of histological grade.</p>","PeriodicalId":53204,"journal":{"name":"Clinical Pathology","volume":" ","pages":"2632010X221129242"},"PeriodicalIF":1.9000,"publicationDate":"2022-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/91/8b/10.1177_2632010X221129242.PMC9608027.pdf","citationCount":"0","resultStr":"{\"title\":\"IGH/BCL2 Status Better Predicts Clinico-Pathological Behavior in Primary Splenic Follicular Lymphoma than Histological Grade and Other Molecular Markers.\",\"authors\":\"Cherian Verghese, Weihong Li, Nanuli Gvazava, Emmanouil Alimpertis, Navkirat Kahlon, Hongliu Sun, Robert Booth\",\"doi\":\"10.1177/2632010X221129242\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Splenic lymphoma may be primary or secondary. Primary splenic lymphoma's are rare and usually of follicular cell origin representing <1% of Non-Hodgkin's Lymphoma's. Most are secondary with 35% representing Marginal Cell sub-type with the rest being Diffuse Large B-Cell Lymphoma's. Unlike the uniformly aggressive clinical course of Diffuse Large B-Cell Lymphoma's, biological behavior of Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma remains less well defined. We present here a solitary splenic mass confirmed as Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma after a diagnostic splenectomy. Biopsy revealed monomorphic small lymphoid cells with low grade mitotic activity. Flow cytometry showed a lambda restricted population of B-Cells displaying dim CD19 and CD10. The cells were negative for CD5, CD11c, and CD103. FISH was negative for IGH/BCL2 fusion unlike nodal Follicular Lymphoma's which are usually positive for this translocation. Evidence from this case and a review of literature support the finding that Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma is less likely to have the classic IGH-BCL2 fusion and the associated chromosomal 14;18 translocation. This profile is associated with less aggressive clinical behavior even when histopathology represents a high-grade pattern. In such cases splenectomy alone is adequate for localized disease when negative for IGH/BCL2 fusion regardless of histological grade.</p>\",\"PeriodicalId\":53204,\"journal\":{\"name\":\"Clinical Pathology\",\"volume\":\" \",\"pages\":\"2632010X221129242\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2022-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/91/8b/10.1177_2632010X221129242.PMC9608027.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pathology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2632010X221129242\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PATHOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2632010X221129242","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PATHOLOGY","Score":null,"Total":0}
IGH/BCL2 Status Better Predicts Clinico-Pathological Behavior in Primary Splenic Follicular Lymphoma than Histological Grade and Other Molecular Markers.
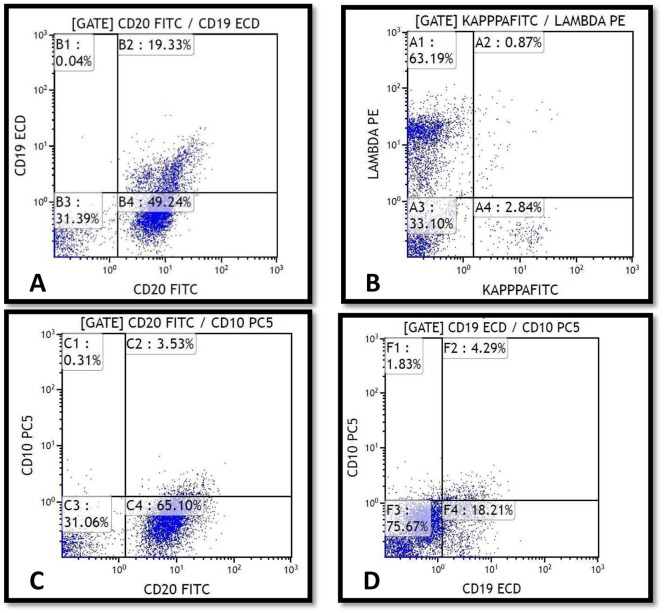
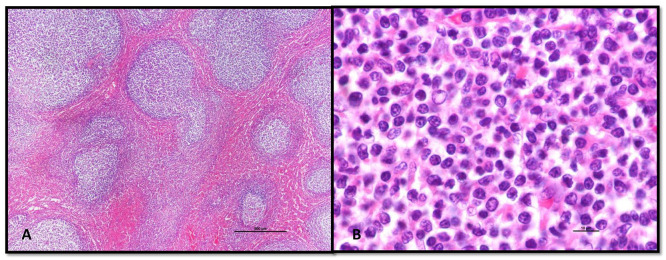
Splenic lymphoma may be primary or secondary. Primary splenic lymphoma's are rare and usually of follicular cell origin representing <1% of Non-Hodgkin's Lymphoma's. Most are secondary with 35% representing Marginal Cell sub-type with the rest being Diffuse Large B-Cell Lymphoma's. Unlike the uniformly aggressive clinical course of Diffuse Large B-Cell Lymphoma's, biological behavior of Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma remains less well defined. We present here a solitary splenic mass confirmed as Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma after a diagnostic splenectomy. Biopsy revealed monomorphic small lymphoid cells with low grade mitotic activity. Flow cytometry showed a lambda restricted population of B-Cells displaying dim CD19 and CD10. The cells were negative for CD5, CD11c, and CD103. FISH was negative for IGH/BCL2 fusion unlike nodal Follicular Lymphoma's which are usually positive for this translocation. Evidence from this case and a review of literature support the finding that Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma is less likely to have the classic IGH-BCL2 fusion and the associated chromosomal 14;18 translocation. This profile is associated with less aggressive clinical behavior even when histopathology represents a high-grade pattern. In such cases splenectomy alone is adequate for localized disease when negative for IGH/BCL2 fusion regardless of histological grade.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
