{"title":"合并症负担对心脏植入式电子设备结果的影响。","authors":"Temitope Ajibawo, Oluwatimilehin Okunowo, Adeniyi Okunade","doi":"10.1177/11795468221108212","DOIUrl":null,"url":null,"abstract":"Background: There is limited data on the impact of comorbidity burden on clinical outcomes of patients undergoing cardiac implantable electronic devices (CIED) implantation. Objectives: Our aim was to assess trends in CIED implantations and explore the relationship between comorbidity burden and outcomes in patients undergoing de novo implantations. Methods: Using the National Inpatient Sample database from 2000 to 2014, we identified adults ⩾18 years undergoing de novo CIED procedures. Comorbidity burden was assessed by Charlson comorbidity Index (CCI), and patients were classified into 4 categories based on their CCI scores (CCI = 0, CCI = 1, CCI = 2, CCI ⩾3). Annual implantation trends were evaluated. Logistic regression was conducted to measure the association between categorized comorbidity burden and outcomes. Results: A total of 3 103 796 de-novo CIED discharge records were identified from the NIS database. About 22.4% had a CCI score of 0, 28.2% had a CCI score of 1, 22% had a CCI score of 2, and 27.4 % had a CCI score ⩾3. Annual de-novo CIED implantations peaked in 2006 and declined steadily from 2010 to 2014. Compared to CCI 0, CCI ⩾3 was independently associated with increased odds of in-hospital mortality, bleeding, pericardial, and cardiac complications (all P < .05). Length of stay and hospital charges increased with increasing comorbidity burden. Conclusions: CCI is a significant predictor of adverse outcomes after CIED implantation. Therefore, comorbidity burden needs to be considered in the decision-making process for CIED implant candidates.","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":" ","pages":"11795468221108212"},"PeriodicalIF":3.3000,"publicationDate":"2022-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bf/f6/10.1177_11795468221108212.PMC9247999.pdf","citationCount":"1","resultStr":"{\"title\":\"Impact of Comorbidity Burden on Cardiac Implantable Electronic Devices Outcomes.\",\"authors\":\"Temitope Ajibawo, Oluwatimilehin Okunowo, Adeniyi Okunade\",\"doi\":\"10.1177/11795468221108212\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Background: There is limited data on the impact of comorbidity burden on clinical outcomes of patients undergoing cardiac implantable electronic devices (CIED) implantation. Objectives: Our aim was to assess trends in CIED implantations and explore the relationship between comorbidity burden and outcomes in patients undergoing de novo implantations. Methods: Using the National Inpatient Sample database from 2000 to 2014, we identified adults ⩾18 years undergoing de novo CIED procedures. Comorbidity burden was assessed by Charlson comorbidity Index (CCI), and patients were classified into 4 categories based on their CCI scores (CCI = 0, CCI = 1, CCI = 2, CCI ⩾3). Annual implantation trends were evaluated. Logistic regression was conducted to measure the association between categorized comorbidity burden and outcomes. Results: A total of 3 103 796 de-novo CIED discharge records were identified from the NIS database. About 22.4% had a CCI score of 0, 28.2% had a CCI score of 1, 22% had a CCI score of 2, and 27.4 % had a CCI score ⩾3. Annual de-novo CIED implantations peaked in 2006 and declined steadily from 2010 to 2014. Compared to CCI 0, CCI ⩾3 was independently associated with increased odds of in-hospital mortality, bleeding, pericardial, and cardiac complications (all P < .05). Length of stay and hospital charges increased with increasing comorbidity burden. Conclusions: CCI is a significant predictor of adverse outcomes after CIED implantation. Therefore, comorbidity burden needs to be considered in the decision-making process for CIED implant candidates.\",\"PeriodicalId\":10419,\"journal\":{\"name\":\"Clinical Medicine Insights. Cardiology\",\"volume\":\" \",\"pages\":\"11795468221108212\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2022-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bf/f6/10.1177_11795468221108212.PMC9247999.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11795468221108212\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795468221108212","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
摘要
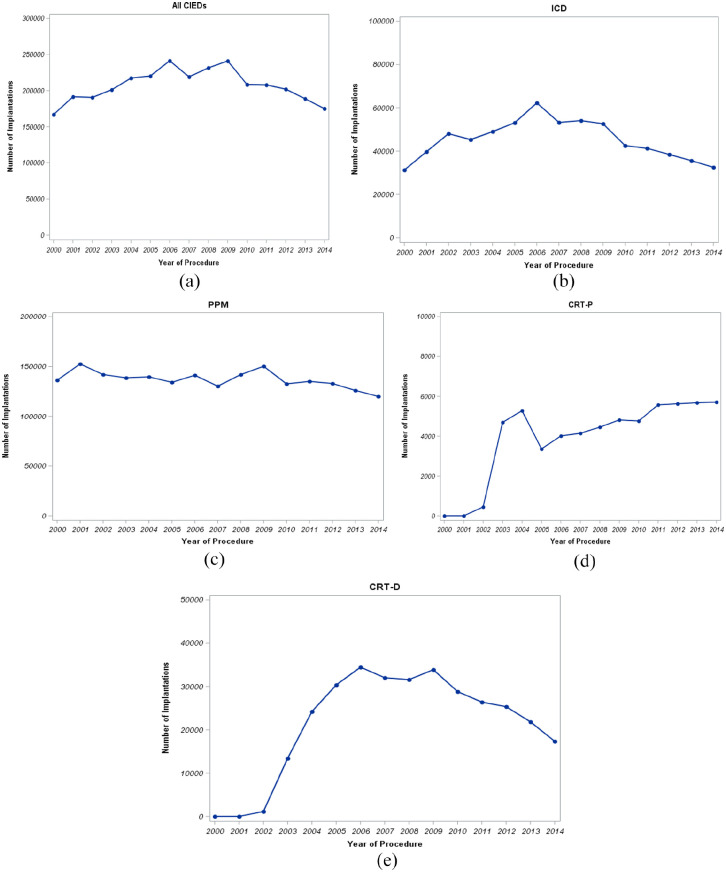
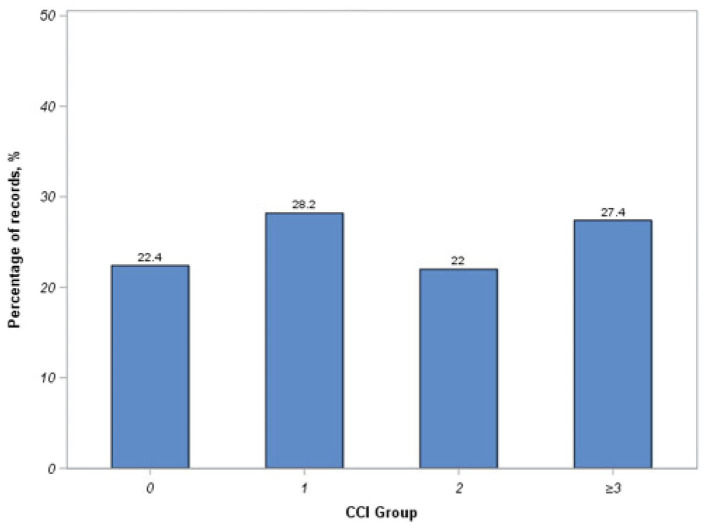
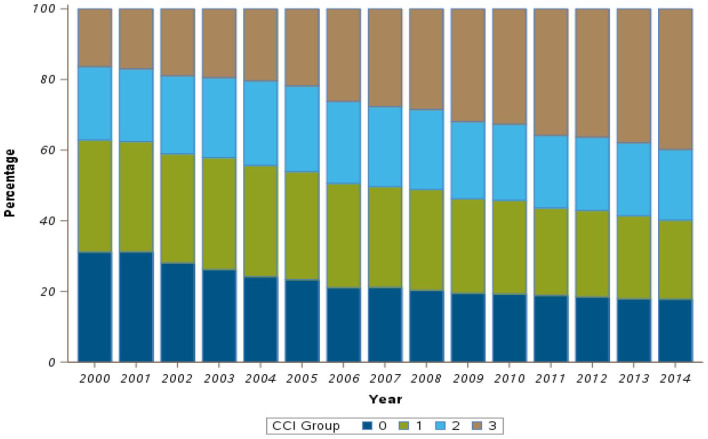
背景:关于合并症负担对心脏植入式电子装置(CIED)植入术患者临床结果影响的数据有限。目的:我们的目的是评估CIED植入的趋势,并探讨接受重新植入的患者的合并症负担和结果之间的关系。方法:使用2000年至2014年的国家住院患者样本数据库,我们确定了接受新生CIED手术的未满18岁的成年人。通过Charlson合并症指数(CCI)评估合并症负担,并根据其CCI评分将患者分为4类(CCI = 0, CCI = 1, CCI = 2, CCI大于或等于3)。评估年度种植趋势。采用逻辑回归来衡量分类共病负担与结局之间的关系。结果:在NIS数据库中共检索到3 103 796例重新诊断的CIED出院记录。约22.4%的CCI得分为0,28.2%的CCI得分为1,22%的CCI得分为2,27.4%的CCI得分大于或等于3。每年重新植入的CIED在2006年达到顶峰,从2010年到2014年稳步下降。与CCI 0相比,CCI小于3与院内死亡率、出血、心包和心脏并发症的几率增加独立相关(所有P结论:CCI是CIED植入后不良结果的重要预测因子。因此,在选择CIED种植体候选人时,需要考虑合并症负担。
Impact of Comorbidity Burden on Cardiac Implantable Electronic Devices Outcomes.
Background: There is limited data on the impact of comorbidity burden on clinical outcomes of patients undergoing cardiac implantable electronic devices (CIED) implantation. Objectives: Our aim was to assess trends in CIED implantations and explore the relationship between comorbidity burden and outcomes in patients undergoing de novo implantations. Methods: Using the National Inpatient Sample database from 2000 to 2014, we identified adults ⩾18 years undergoing de novo CIED procedures. Comorbidity burden was assessed by Charlson comorbidity Index (CCI), and patients were classified into 4 categories based on their CCI scores (CCI = 0, CCI = 1, CCI = 2, CCI ⩾3). Annual implantation trends were evaluated. Logistic regression was conducted to measure the association between categorized comorbidity burden and outcomes. Results: A total of 3 103 796 de-novo CIED discharge records were identified from the NIS database. About 22.4% had a CCI score of 0, 28.2% had a CCI score of 1, 22% had a CCI score of 2, and 27.4 % had a CCI score ⩾3. Annual de-novo CIED implantations peaked in 2006 and declined steadily from 2010 to 2014. Compared to CCI 0, CCI ⩾3 was independently associated with increased odds of in-hospital mortality, bleeding, pericardial, and cardiac complications (all P < .05). Length of stay and hospital charges increased with increasing comorbidity burden. Conclusions: CCI is a significant predictor of adverse outcomes after CIED implantation. Therefore, comorbidity burden needs to be considered in the decision-making process for CIED implant candidates.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
