{"title":"单侧和双侧核间眼麻痹的保守和手术治疗回顾性分析。","authors":"Joshua Simmons, Martin Rhodes","doi":"10.22599/bioj.280","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To report the outcomes of the natural progression and ophthalmic treatment of patients reviewed in a tertiary hospital trust with unilateral or bilateral internuclear ophthalmoplegia.</p><p><strong>Method: </strong>A retrospective case note analysis was performed and 33 patients diagnosed with unilateral or bilateral internuclear ophthalmoplegia (INO) were identified. The diagnosis, aetiology, presence of diplopia, ophthalmic management options and progression were recorded and analysed. This included both conservative and surgical management.</p><p><strong>Results: </strong>The most common aetiologies of INO within this cohort were stroke/ischaemic (69.7%) and multiple sclerosis (MS) (30.3%). Unilateral INO was more prevalent than bilateral INO, with 20 cases (60.6%) compared to 13 cases (39.4%), respectively. A higher proportion of unilateral INO were attributed to stroke (90%) whilst a higher proportion of bilateral INO were attributed to MS (61.5%). The most prescribed management at primary assessment was occlusion (45.5%) and prisms (24.2%). Some patients required no orthoptic intervention (30.3%). Two patients had surgical management of strabismus secondary to bilateral INO.</p><p><strong>Conclusion: </strong>Occlusion was the most common form of management for symptomatic relief of diplopia. Patients who presented at the first visit with no symptoms were unlikely to need any orthoptic intervention. Of the two patients who went on to require surgical intervention, restoration of binocular single vision (BSV) was achieved post-operatively with the use of a Fresnel prism. However, the differences in both surgical technique and number of surgeries required make this difficult to generalise. Additional research is needed to further explore the surgical management of INO.</p>","PeriodicalId":36083,"journal":{"name":"British and Irish Orthoptic Journal","volume":" ","pages":"152-158"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9650975/pdf/","citationCount":"0","resultStr":"{\"title\":\"Conservative and Surgical Management of Unilateral and Bilateral Internuclear Ophthalmoplegia (INO)-A Retrospective Analysis.\",\"authors\":\"Joshua Simmons, Martin Rhodes\",\"doi\":\"10.22599/bioj.280\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim: </strong>To report the outcomes of the natural progression and ophthalmic treatment of patients reviewed in a tertiary hospital trust with unilateral or bilateral internuclear ophthalmoplegia.</p><p><strong>Method: </strong>A retrospective case note analysis was performed and 33 patients diagnosed with unilateral or bilateral internuclear ophthalmoplegia (INO) were identified. The diagnosis, aetiology, presence of diplopia, ophthalmic management options and progression were recorded and analysed. This included both conservative and surgical management.</p><p><strong>Results: </strong>The most common aetiologies of INO within this cohort were stroke/ischaemic (69.7%) and multiple sclerosis (MS) (30.3%). Unilateral INO was more prevalent than bilateral INO, with 20 cases (60.6%) compared to 13 cases (39.4%), respectively. A higher proportion of unilateral INO were attributed to stroke (90%) whilst a higher proportion of bilateral INO were attributed to MS (61.5%). The most prescribed management at primary assessment was occlusion (45.5%) and prisms (24.2%). Some patients required no orthoptic intervention (30.3%). Two patients had surgical management of strabismus secondary to bilateral INO.</p><p><strong>Conclusion: </strong>Occlusion was the most common form of management for symptomatic relief of diplopia. Patients who presented at the first visit with no symptoms were unlikely to need any orthoptic intervention. Of the two patients who went on to require surgical intervention, restoration of binocular single vision (BSV) was achieved post-operatively with the use of a Fresnel prism. However, the differences in both surgical technique and number of surgeries required make this difficult to generalise. Additional research is needed to further explore the surgical management of INO.</p>\",\"PeriodicalId\":36083,\"journal\":{\"name\":\"British and Irish Orthoptic Journal\",\"volume\":\" \",\"pages\":\"152-158\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-11-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9650975/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"British and Irish Orthoptic Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22599/bioj.280\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"British and Irish Orthoptic Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22599/bioj.280","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Conservative and Surgical Management of Unilateral and Bilateral Internuclear Ophthalmoplegia (INO)-A Retrospective Analysis.
Aim: To report the outcomes of the natural progression and ophthalmic treatment of patients reviewed in a tertiary hospital trust with unilateral or bilateral internuclear ophthalmoplegia.
Method: A retrospective case note analysis was performed and 33 patients diagnosed with unilateral or bilateral internuclear ophthalmoplegia (INO) were identified. The diagnosis, aetiology, presence of diplopia, ophthalmic management options and progression were recorded and analysed. This included both conservative and surgical management.
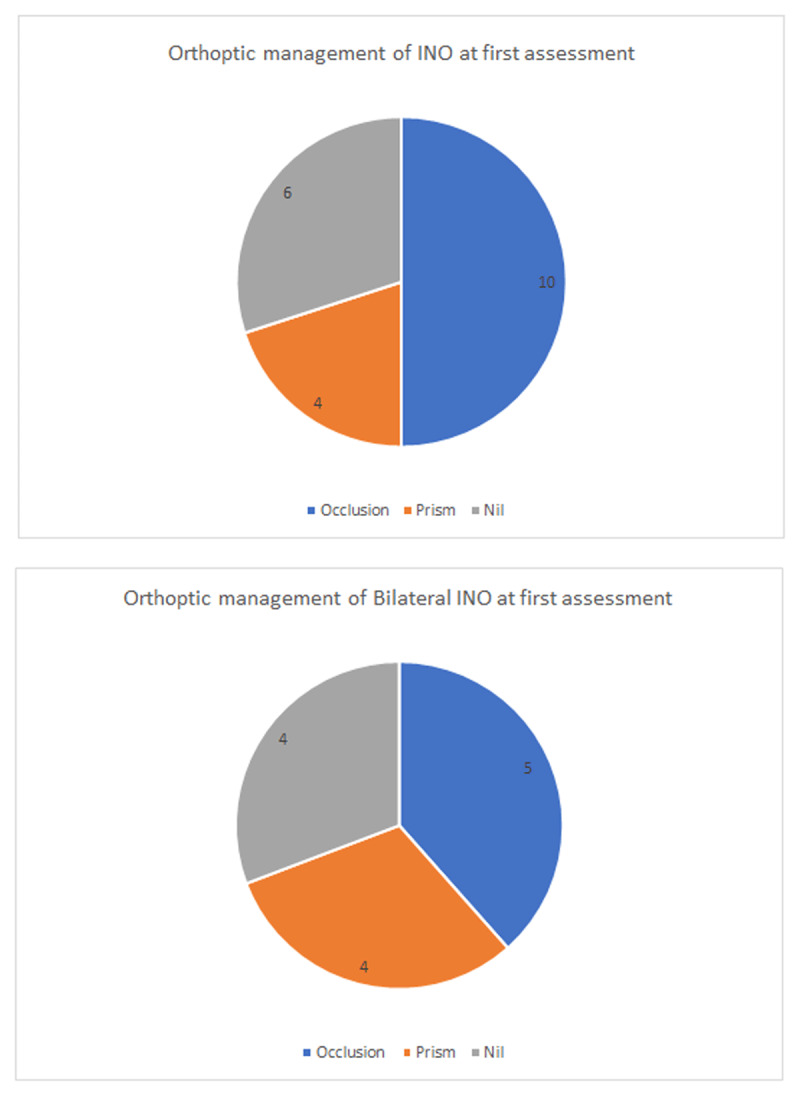
Results: The most common aetiologies of INO within this cohort were stroke/ischaemic (69.7%) and multiple sclerosis (MS) (30.3%). Unilateral INO was more prevalent than bilateral INO, with 20 cases (60.6%) compared to 13 cases (39.4%), respectively. A higher proportion of unilateral INO were attributed to stroke (90%) whilst a higher proportion of bilateral INO were attributed to MS (61.5%). The most prescribed management at primary assessment was occlusion (45.5%) and prisms (24.2%). Some patients required no orthoptic intervention (30.3%). Two patients had surgical management of strabismus secondary to bilateral INO.
Conclusion: Occlusion was the most common form of management for symptomatic relief of diplopia. Patients who presented at the first visit with no symptoms were unlikely to need any orthoptic intervention. Of the two patients who went on to require surgical intervention, restoration of binocular single vision (BSV) was achieved post-operatively with the use of a Fresnel prism. However, the differences in both surgical technique and number of surgeries required make this difficult to generalise. Additional research is needed to further explore the surgical management of INO.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
