Gregory T Carroll, David L Kirschman, Angela Mammana
{"title":"手术室内二氧化碳浓度的增加与在场医护人员的数量有关:必须有意识地控制人群。","authors":"Gregory T Carroll, David L Kirschman, Angela Mammana","doi":"10.1186/s13037-022-00343-8","DOIUrl":null,"url":null,"abstract":"<p><p>The air in an operating room becomes more contaminated as the occupancy of the room increases. Individuals residing in a room can potentially emit infectious agents. In order to inhibit and better understand the epidemiology of surgical site infections, it is important to develop procedures to track room occupancy level and respiration. Exhaled CO<sub>2</sub> provides a respiratory byproduct that can be tracked with IR light and is associated with human occupancy. Exhaled CO<sub>2</sub> can also be used as an indirect measure of the potential release and level of infectious airborne agents. We show that non-dispersive infrared CO<sub>2</sub> sensors can be used to detect CO<sub>2</sub> in operating room air flow conditions of 20 air changes per hour and a positive pressure of 0.03 in. H<sub>2</sub>O. The CO<sub>2</sub> concentration increased consecutively for occupation levels of one to four individuals, from approximately 65 ppm above the background level when one individual occupied the operating room for twenty minutes to approximately 300 ppm above the background when four individuals were present for twenty minutes. The amount of CO<sub>2</sub> detected increases as the number of occupants increase, the activity level increases, the residency time increases and when the ventilation level is reduced.</p>","PeriodicalId":2,"journal":{"name":"ACS Applied Bio Materials","volume":" ","pages":"35"},"PeriodicalIF":4.7000,"publicationDate":"2022-11-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9672642/pdf/","citationCount":"0","resultStr":"{\"title\":\"Increased CO<sub>2</sub> levels in the operating room correlate with the number of healthcare workers present: an imperative for intentional crowd control.\",\"authors\":\"Gregory T Carroll, David L Kirschman, Angela Mammana\",\"doi\":\"10.1186/s13037-022-00343-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The air in an operating room becomes more contaminated as the occupancy of the room increases. Individuals residing in a room can potentially emit infectious agents. In order to inhibit and better understand the epidemiology of surgical site infections, it is important to develop procedures to track room occupancy level and respiration. Exhaled CO<sub>2</sub> provides a respiratory byproduct that can be tracked with IR light and is associated with human occupancy. Exhaled CO<sub>2</sub> can also be used as an indirect measure of the potential release and level of infectious airborne agents. We show that non-dispersive infrared CO<sub>2</sub> sensors can be used to detect CO<sub>2</sub> in operating room air flow conditions of 20 air changes per hour and a positive pressure of 0.03 in. H<sub>2</sub>O. The CO<sub>2</sub> concentration increased consecutively for occupation levels of one to four individuals, from approximately 65 ppm above the background level when one individual occupied the operating room for twenty minutes to approximately 300 ppm above the background when four individuals were present for twenty minutes. The amount of CO<sub>2</sub> detected increases as the number of occupants increase, the activity level increases, the residency time increases and when the ventilation level is reduced.</p>\",\"PeriodicalId\":2,\"journal\":{\"name\":\"ACS Applied Bio Materials\",\"volume\":\" \",\"pages\":\"35\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2022-11-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9672642/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACS Applied Bio Materials\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13037-022-00343-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MATERIALS SCIENCE, BIOMATERIALS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Bio Materials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13037-022-00343-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MATERIALS SCIENCE, BIOMATERIALS","Score":null,"Total":0}
Increased CO2 levels in the operating room correlate with the number of healthcare workers present: an imperative for intentional crowd control.
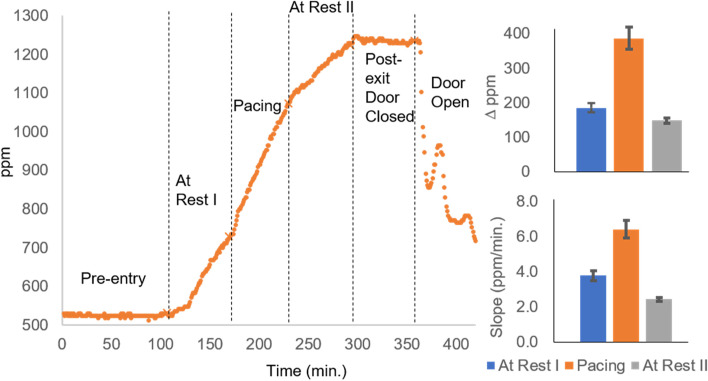
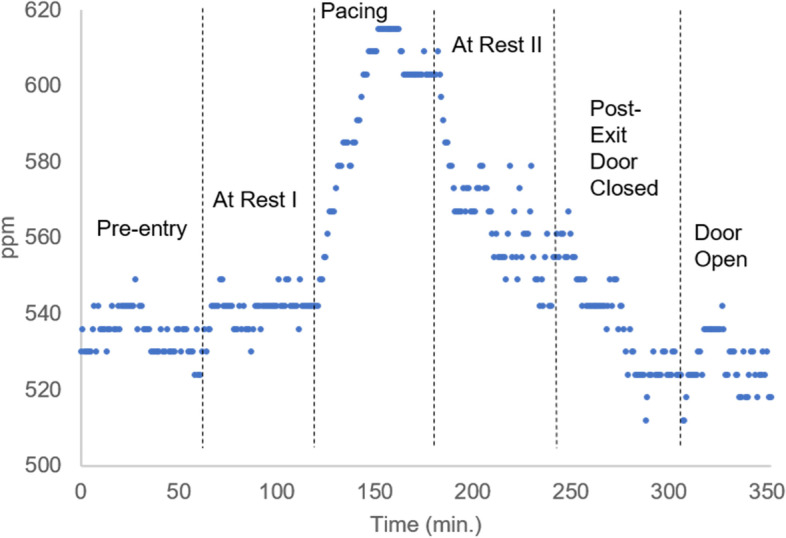
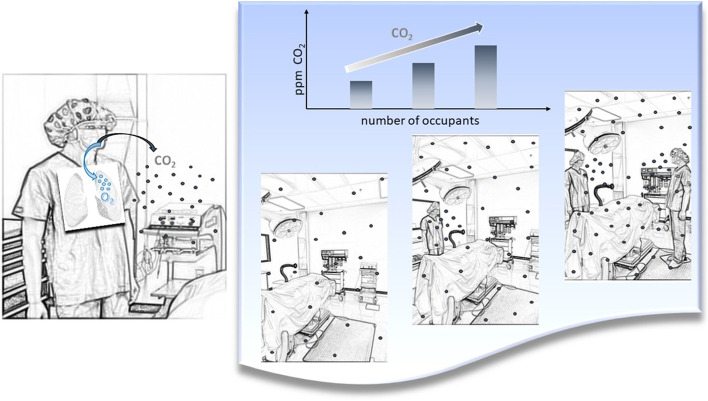
The air in an operating room becomes more contaminated as the occupancy of the room increases. Individuals residing in a room can potentially emit infectious agents. In order to inhibit and better understand the epidemiology of surgical site infections, it is important to develop procedures to track room occupancy level and respiration. Exhaled CO2 provides a respiratory byproduct that can be tracked with IR light and is associated with human occupancy. Exhaled CO2 can also be used as an indirect measure of the potential release and level of infectious airborne agents. We show that non-dispersive infrared CO2 sensors can be used to detect CO2 in operating room air flow conditions of 20 air changes per hour and a positive pressure of 0.03 in. H2O. The CO2 concentration increased consecutively for occupation levels of one to four individuals, from approximately 65 ppm above the background level when one individual occupied the operating room for twenty minutes to approximately 300 ppm above the background when four individuals were present for twenty minutes. The amount of CO2 detected increases as the number of occupants increase, the activity level increases, the residency time increases and when the ventilation level is reduced.
期刊介绍:
ACS Applied Bio Materials is an interdisciplinary journal publishing original research covering all aspects of biomaterials and biointerfaces including and beyond the traditional biosensing, biomedical and therapeutic applications.
The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrates knowledge in the areas of materials, engineering, physics, bioscience, and chemistry into important bio applications. The journal is specifically interested in work that addresses the relationship between structure and function and assesses the stability and degradation of materials under relevant environmental and biological conditions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
