David W Liu, Sara Martinez Martos, Yifei Dai, Elaine M Beller
{"title":"股骨髁间切迹是全膝关节置换术中股骨远端切除深度的准确标志。","authors":"David W Liu, Sara Martinez Martos, Yifei Dai, Elaine M Beller","doi":"10.1186/s43019-022-00159-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Conventionally, the depth of distal femoral resection in total knee arthroplasty is referenced from the most prominent distal femoral condyle. This surgical technique does not consider pathological alterations of articular surfaces or severity of knee deformity. It has been hypothesized that the femoral intercondylar notch is a clinically reliable and more accurate alternative landmark for the resection depth of the distal femur in primary total knee arthroplasty.</p><p><strong>Methods: </strong>The resection depths of the distal femur at the medial and lateral femoral condyles and intercondylar notch were measured using computer navigation in 406 total knee arthroplasties. Variability between the bone resection depths was analyzed by standard deviation, 95% confidence interval and variance. Clinical follow-up of outcome to a minimum of 12 months was performed to further inform and validate the analysis.</p><p><strong>Results: </strong>Mean resection depth of the medial condyle was 10.7 mm, of the lateral condyle 7.9 mm and of the femoral intercondylar notch 1.9 mm. The femoral intercondylar notch had the lowest variance in resection depth among the three landmarks assessed, with a variance of 1.7 mm<sup>2</sup> compared to 2.8 mm<sup>2</sup> for the medial femoral condyle and 5.1 mm<sup>2</sup> for the lateral femoral condyle. The intercondylar notch reference had the lowest standard deviation and 95% confidence interval. The resection depth referencing the notch was not sensitive to the degree of flexion contracture pre-operatively, whereas the medial and lateral condyles were. For varus deformed knees, distal femoral resection depth at the notch averaged 2 mm, which corresponds to the femoral prosthesis thickness at the intercondylar region, while for valgus deformed knees, the resection was flush with the intercondylar notch.</p><p><strong>Conclusions: </strong>The femoral intercondylar notch is a clinically practical and reproducible landmark for appropriate and accurate resection depth of the distal femur in primary total knee arthroplasty.</p><p><strong>Level of evidence: </strong>Level III: Retrospective cohort study.</p>","PeriodicalId":17886,"journal":{"name":"Knee Surgery & Related Research","volume":" ","pages":"32"},"PeriodicalIF":4.4000,"publicationDate":"2022-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9264514/pdf/","citationCount":"2","resultStr":"{\"title\":\"The femoral intercondylar notch is an accurate landmark for the resection depth of the distal femur in total knee arthroplasty.\",\"authors\":\"David W Liu, Sara Martinez Martos, Yifei Dai, Elaine M Beller\",\"doi\":\"10.1186/s43019-022-00159-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Conventionally, the depth of distal femoral resection in total knee arthroplasty is referenced from the most prominent distal femoral condyle. This surgical technique does not consider pathological alterations of articular surfaces or severity of knee deformity. It has been hypothesized that the femoral intercondylar notch is a clinically reliable and more accurate alternative landmark for the resection depth of the distal femur in primary total knee arthroplasty.</p><p><strong>Methods: </strong>The resection depths of the distal femur at the medial and lateral femoral condyles and intercondylar notch were measured using computer navigation in 406 total knee arthroplasties. Variability between the bone resection depths was analyzed by standard deviation, 95% confidence interval and variance. Clinical follow-up of outcome to a minimum of 12 months was performed to further inform and validate the analysis.</p><p><strong>Results: </strong>Mean resection depth of the medial condyle was 10.7 mm, of the lateral condyle 7.9 mm and of the femoral intercondylar notch 1.9 mm. The femoral intercondylar notch had the lowest variance in resection depth among the three landmarks assessed, with a variance of 1.7 mm<sup>2</sup> compared to 2.8 mm<sup>2</sup> for the medial femoral condyle and 5.1 mm<sup>2</sup> for the lateral femoral condyle. The intercondylar notch reference had the lowest standard deviation and 95% confidence interval. The resection depth referencing the notch was not sensitive to the degree of flexion contracture pre-operatively, whereas the medial and lateral condyles were. For varus deformed knees, distal femoral resection depth at the notch averaged 2 mm, which corresponds to the femoral prosthesis thickness at the intercondylar region, while for valgus deformed knees, the resection was flush with the intercondylar notch.</p><p><strong>Conclusions: </strong>The femoral intercondylar notch is a clinically practical and reproducible landmark for appropriate and accurate resection depth of the distal femur in primary total knee arthroplasty.</p><p><strong>Level of evidence: </strong>Level III: Retrospective cohort study.</p>\",\"PeriodicalId\":17886,\"journal\":{\"name\":\"Knee Surgery & Related Research\",\"volume\":\" \",\"pages\":\"32\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2022-07-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9264514/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Knee Surgery & Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s43019-022-00159-x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery & Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-022-00159-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
The femoral intercondylar notch is an accurate landmark for the resection depth of the distal femur in total knee arthroplasty.
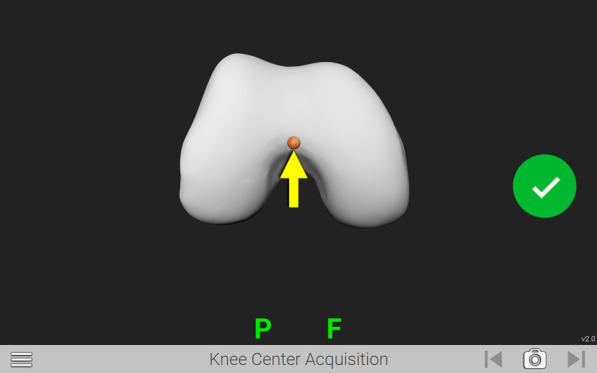
Introduction: Conventionally, the depth of distal femoral resection in total knee arthroplasty is referenced from the most prominent distal femoral condyle. This surgical technique does not consider pathological alterations of articular surfaces or severity of knee deformity. It has been hypothesized that the femoral intercondylar notch is a clinically reliable and more accurate alternative landmark for the resection depth of the distal femur in primary total knee arthroplasty.
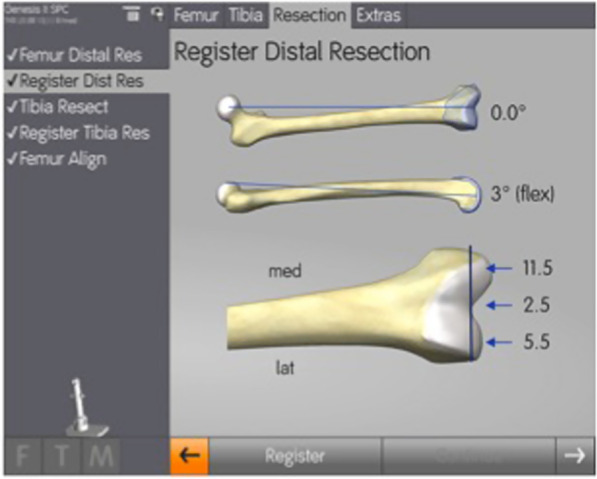
Methods: The resection depths of the distal femur at the medial and lateral femoral condyles and intercondylar notch were measured using computer navigation in 406 total knee arthroplasties. Variability between the bone resection depths was analyzed by standard deviation, 95% confidence interval and variance. Clinical follow-up of outcome to a minimum of 12 months was performed to further inform and validate the analysis.
Results: Mean resection depth of the medial condyle was 10.7 mm, of the lateral condyle 7.9 mm and of the femoral intercondylar notch 1.9 mm. The femoral intercondylar notch had the lowest variance in resection depth among the three landmarks assessed, with a variance of 1.7 mm2 compared to 2.8 mm2 for the medial femoral condyle and 5.1 mm2 for the lateral femoral condyle. The intercondylar notch reference had the lowest standard deviation and 95% confidence interval. The resection depth referencing the notch was not sensitive to the degree of flexion contracture pre-operatively, whereas the medial and lateral condyles were. For varus deformed knees, distal femoral resection depth at the notch averaged 2 mm, which corresponds to the femoral prosthesis thickness at the intercondylar region, while for valgus deformed knees, the resection was flush with the intercondylar notch.
Conclusions: The femoral intercondylar notch is a clinically practical and reproducible landmark for appropriate and accurate resection depth of the distal femur in primary total knee arthroplasty.
Level of evidence: Level III: Retrospective cohort study.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
