Young Rong Kim MD , Ha-Jin Chun , Jung Yeon Heo MD, PhD , Jin Sae Yoo MD , Young Hwa Choi MD, PhD , Eun Jin Kim MD
{"title":"浓度-时间曲线引导下监测面积对韩国耐甲氧西林金黄色葡萄球菌血症患者万古霉素肾毒性及治疗效果的影响","authors":"Young Rong Kim MD , Ha-Jin Chun , Jung Yeon Heo MD, PhD , Jin Sae Yoo MD , Young Hwa Choi MD, PhD , Eun Jin Kim MD","doi":"10.1016/j.curtheres.2022.100687","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Current guidelines for the therapeutic monitoring of vancomycin recommend dosing based on the area under the concentration-time curve (AUC) to achieve clinical efficacy while reducing nephrotoxicity. Although a wide range of nephrotoxicity thresholds have been reported, few studies have documented clinical outcomes based on AUC-guided vancomycin dosing in Korea.</p></div><div><h3>Objective</h3><p>The aim of the study was to evaluate whether a relationship exists between AUC and treatment outcomes in vancomycin treated patients in methicillin-resistant <em>Staphylococcus aureus</em> bacteremia. Furthermore, this study tries to estimate AUC threshold for treatment failure and nephrotoxicity.</p></div><div><h3>Methods</h3><p>The records of adult patients with methicillin-resistant <em>Staphylococcus aureus</em> bacteremia treated with vancomycin for ≥72 hours without dialysis between April 2013 and April 2021, were reviewed retrospectively. Treatment success was defined as defervescence and blood culture sterilization by day 7. Nephrotoxicity was defined as an increase in serum creatinine levels ≥0.3 mg/dL or a 50% increase from baseline on 2 consecutive days. Bayesian estimation was used to predict individual vancomycin AUC. Both classification and regression tree and receiver operating characteristic curve analyses were performed to estimate the optimal AUC thresholds for vancomycin efficacy and nephrotoxicity.</p></div><div><h3>Results</h3><p>Of 118 patients, 61 (51.7%) experienced treatment failure and 42 (35.6%) developed acute kidney injury. The vancomycin AUC threshold for predicting acute kidney injury was 615.0 mg· hr/L. In the multivariate analysis, AUC ≥615.0 mg· hr/L was a significant risk factor for nephrotoxicity (adjusted odds ratio [aOR] = 5.24; 95% CI, 1.8–14.65). The lower threshold for treatment failure was not defined because it was not statistically significant. Risk factors for treatment failure included low body mass index (aOR = 0.82; 95% CI, 0.70–0.96), severity of acute illness represented by complicated infection (aOR = 77.56; 95% CI, 16.7–359.4) and comorbidities, such as solid organ tumors (aOR = 6.61; 95% CI, 1.19–36.81) and cerebrovascular disease (aOR = 6.05; 95% CI, 1.17–31.23).</p></div><div><h3>Conclusions</h3><p>Although AUC-guided vancomycin dosing was associated with a reduced risk of acute kidney injury, its ability to predict clinical outcomes was modest. Further studies are needed to define the AUC therapeutic range to maximize efficacy and minimize nephrotoxicity. (<em>Curr Ther Res Clin Exp.</em> 2023; 83:XXX–XXX)</p></div>","PeriodicalId":10920,"journal":{"name":"Current Therapeutic Research-clinical and Experimental","volume":"97 ","pages":"Article 100687"},"PeriodicalIF":1.5000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/25/55/main.PMC9691871.pdf","citationCount":"1","resultStr":"{\"title\":\"Impact of Area Under the Concentration-Time Curve-Guided Monitoring on Vancomycin Nephrotoxicity and Treatment Outcomes in Methicillin-Resistant Staphylococcus Aureus Bacteremia in Korean Patients\",\"authors\":\"Young Rong Kim MD , Ha-Jin Chun , Jung Yeon Heo MD, PhD , Jin Sae Yoo MD , Young Hwa Choi MD, PhD , Eun Jin Kim MD\",\"doi\":\"10.1016/j.curtheres.2022.100687\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Current guidelines for the therapeutic monitoring of vancomycin recommend dosing based on the area under the concentration-time curve (AUC) to achieve clinical efficacy while reducing nephrotoxicity. Although a wide range of nephrotoxicity thresholds have been reported, few studies have documented clinical outcomes based on AUC-guided vancomycin dosing in Korea.</p></div><div><h3>Objective</h3><p>The aim of the study was to evaluate whether a relationship exists between AUC and treatment outcomes in vancomycin treated patients in methicillin-resistant <em>Staphylococcus aureus</em> bacteremia. Furthermore, this study tries to estimate AUC threshold for treatment failure and nephrotoxicity.</p></div><div><h3>Methods</h3><p>The records of adult patients with methicillin-resistant <em>Staphylococcus aureus</em> bacteremia treated with vancomycin for ≥72 hours without dialysis between April 2013 and April 2021, were reviewed retrospectively. Treatment success was defined as defervescence and blood culture sterilization by day 7. Nephrotoxicity was defined as an increase in serum creatinine levels ≥0.3 mg/dL or a 50% increase from baseline on 2 consecutive days. Bayesian estimation was used to predict individual vancomycin AUC. Both classification and regression tree and receiver operating characteristic curve analyses were performed to estimate the optimal AUC thresholds for vancomycin efficacy and nephrotoxicity.</p></div><div><h3>Results</h3><p>Of 118 patients, 61 (51.7%) experienced treatment failure and 42 (35.6%) developed acute kidney injury. The vancomycin AUC threshold for predicting acute kidney injury was 615.0 mg· hr/L. In the multivariate analysis, AUC ≥615.0 mg· hr/L was a significant risk factor for nephrotoxicity (adjusted odds ratio [aOR] = 5.24; 95% CI, 1.8–14.65). The lower threshold for treatment failure was not defined because it was not statistically significant. Risk factors for treatment failure included low body mass index (aOR = 0.82; 95% CI, 0.70–0.96), severity of acute illness represented by complicated infection (aOR = 77.56; 95% CI, 16.7–359.4) and comorbidities, such as solid organ tumors (aOR = 6.61; 95% CI, 1.19–36.81) and cerebrovascular disease (aOR = 6.05; 95% CI, 1.17–31.23).</p></div><div><h3>Conclusions</h3><p>Although AUC-guided vancomycin dosing was associated with a reduced risk of acute kidney injury, its ability to predict clinical outcomes was modest. Further studies are needed to define the AUC therapeutic range to maximize efficacy and minimize nephrotoxicity. (<em>Curr Ther Res Clin Exp.</em> 2023; 83:XXX–XXX)</p></div>\",\"PeriodicalId\":10920,\"journal\":{\"name\":\"Current Therapeutic Research-clinical and Experimental\",\"volume\":\"97 \",\"pages\":\"Article 100687\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/25/55/main.PMC9691871.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Therapeutic Research-clinical and Experimental\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0011393X22000261\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Therapeutic Research-clinical and Experimental","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0011393X22000261","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Impact of Area Under the Concentration-Time Curve-Guided Monitoring on Vancomycin Nephrotoxicity and Treatment Outcomes in Methicillin-Resistant Staphylococcus Aureus Bacteremia in Korean Patients
Background
Current guidelines for the therapeutic monitoring of vancomycin recommend dosing based on the area under the concentration-time curve (AUC) to achieve clinical efficacy while reducing nephrotoxicity. Although a wide range of nephrotoxicity thresholds have been reported, few studies have documented clinical outcomes based on AUC-guided vancomycin dosing in Korea.
Objective
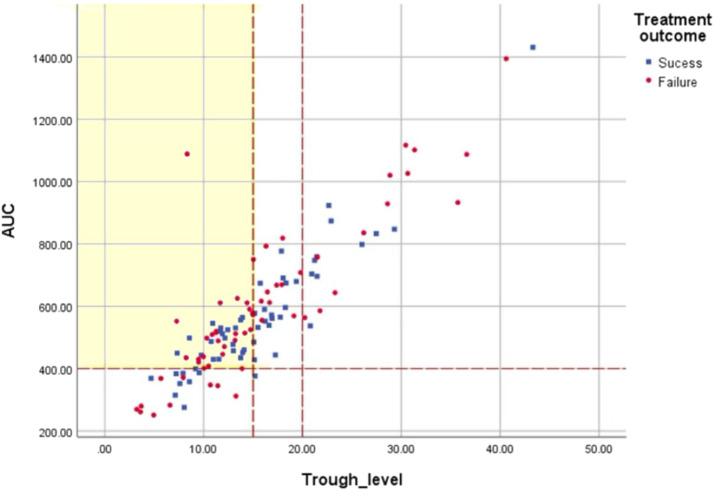
The aim of the study was to evaluate whether a relationship exists between AUC and treatment outcomes in vancomycin treated patients in methicillin-resistant Staphylococcus aureus bacteremia. Furthermore, this study tries to estimate AUC threshold for treatment failure and nephrotoxicity.
Methods
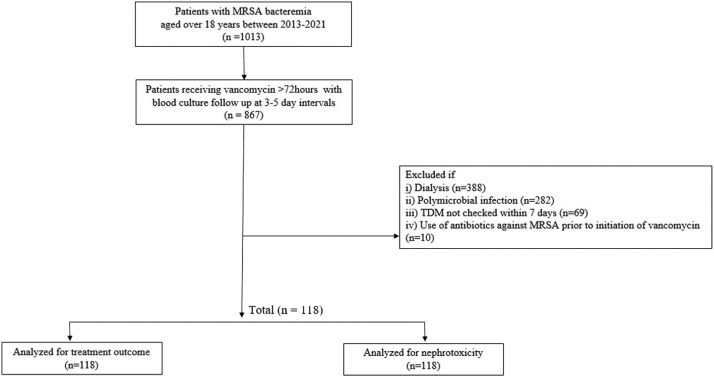
The records of adult patients with methicillin-resistant Staphylococcus aureus bacteremia treated with vancomycin for ≥72 hours without dialysis between April 2013 and April 2021, were reviewed retrospectively. Treatment success was defined as defervescence and blood culture sterilization by day 7. Nephrotoxicity was defined as an increase in serum creatinine levels ≥0.3 mg/dL or a 50% increase from baseline on 2 consecutive days. Bayesian estimation was used to predict individual vancomycin AUC. Both classification and regression tree and receiver operating characteristic curve analyses were performed to estimate the optimal AUC thresholds for vancomycin efficacy and nephrotoxicity.
Results
Of 118 patients, 61 (51.7%) experienced treatment failure and 42 (35.6%) developed acute kidney injury. The vancomycin AUC threshold for predicting acute kidney injury was 615.0 mg· hr/L. In the multivariate analysis, AUC ≥615.0 mg· hr/L was a significant risk factor for nephrotoxicity (adjusted odds ratio [aOR] = 5.24; 95% CI, 1.8–14.65). The lower threshold for treatment failure was not defined because it was not statistically significant. Risk factors for treatment failure included low body mass index (aOR = 0.82; 95% CI, 0.70–0.96), severity of acute illness represented by complicated infection (aOR = 77.56; 95% CI, 16.7–359.4) and comorbidities, such as solid organ tumors (aOR = 6.61; 95% CI, 1.19–36.81) and cerebrovascular disease (aOR = 6.05; 95% CI, 1.17–31.23).
Conclusions
Although AUC-guided vancomycin dosing was associated with a reduced risk of acute kidney injury, its ability to predict clinical outcomes was modest. Further studies are needed to define the AUC therapeutic range to maximize efficacy and minimize nephrotoxicity. (Curr Ther Res Clin Exp. 2023; 83:XXX–XXX)
期刊介绍:
We also encourage the submission of manuscripts presenting preclinical and very preliminary research that may stimulate further investigation of potentially relevant findings, as well as in-depth review articles on specific therapies or disease states, and applied health delivery or pharmacoeconomics.
CTR encourages and supports the submission of manuscripts describing:
• Interventions designed to understand or improve human health, disease treatment or disease prevention;
• Studies that focus on problems that are uncommon in resource-rich countries;
• Research that is "under-published" because of limited access to monetary resources such as English language support and Open Access fees (CTR offers deeply discounted English language editing);
• Republication of articles previously published in non-English journals (eg, evidence-based guidelines) which could be useful if translated into English;
• Preclinical and clinical product development studies that are not pursued for further investigation based upon early phase results.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
