Christian Habib Ayoub, Ali Dakroub, Jose M El-Asmar, Adel Hajj Ali, Hadi Beaini, Suhaib Abdulfattah, Albert El Hajj
{"title":"术前 MELD 评分预测根治性膀胱切除术后的死亡率和不良后果:美国外科学院国家外科质量改进计划分析。","authors":"Christian Habib Ayoub, Ali Dakroub, Jose M El-Asmar, Adel Hajj Ali, Hadi Beaini, Suhaib Abdulfattah, Albert El Hajj","doi":"10.1177/17562872221135944","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The model for end-stage liver disease (MELD) has been widely used to predict the mortality and morbidity of various surgical procedures.</p><p><strong>Objectives: </strong>We aimed to correlate a high preoperative MELD score with adverse 30-day postoperative complications following radical cystectomy.</p><p><strong>Design and methods: </strong>Patients who underwent elective, non-emergency radical cystectomy were identified from the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005 to 2017. Patients were categorized according to a calculated MELD score. The primary outcomes of this study were 30-day postoperative mortality, morbidity, and length of hospital stay following radical cystectomy. For further sensitivity analysis, propensity score matching was used to yield a total of 1387 matched pairs and primary outcomes were also assessed in the matched cohort.</p><p><strong>Results: </strong>Compared with patients with a MELD < 10, those with MELD ⩾ 10 had significantly higher rates of mortality [odds ratio (OR) = 1.71, <i>p =</i> 0.004], major complications (OR = 1.42, <i>p <</i> 0.001), and prolonged hospital stay (OR = 1.29, <i>p <</i> 0.001) on multivariate analysis. Following risk-adjustment for race, propensity-matched groups revealed that patients with MELD score ⩾ 10 were significantly associated with higher mortality (OR = 1.85, <i>p =</i> 0.008), major complications (OR = 1.34, <i>p <</i> 0.001), yet similar length of hospital stay (OR = 1.17, <i>p =</i> 0.072).</p><p><strong>Conclusion: </strong>MELD score ⩾ 10 is associated with higher mortality and morbidity in patients undergoing radical cystectomy compared with lower MELD scores. Risk-stratification using MELD score may assist clinicians in identifying high-risk patients to provide adequate preoperative counseling, optimize perioperative conditions, and even consider nonsurgical alternatives.</p>","PeriodicalId":2,"journal":{"name":"ACS Applied Bio Materials","volume":" ","pages":"17562872221135944"},"PeriodicalIF":4.7000,"publicationDate":"2022-11-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/96/8f/10.1177_17562872221135944.PMC9669693.pdf","citationCount":"0","resultStr":"{\"title\":\"Preoperative MELD score predicts mortality and adverse outcomes following radical cystectomy: analysis of American College of Surgeons National Surgical Quality Improvement Program.\",\"authors\":\"Christian Habib Ayoub, Ali Dakroub, Jose M El-Asmar, Adel Hajj Ali, Hadi Beaini, Suhaib Abdulfattah, Albert El Hajj\",\"doi\":\"10.1177/17562872221135944\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The model for end-stage liver disease (MELD) has been widely used to predict the mortality and morbidity of various surgical procedures.</p><p><strong>Objectives: </strong>We aimed to correlate a high preoperative MELD score with adverse 30-day postoperative complications following radical cystectomy.</p><p><strong>Design and methods: </strong>Patients who underwent elective, non-emergency radical cystectomy were identified from the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005 to 2017. Patients were categorized according to a calculated MELD score. The primary outcomes of this study were 30-day postoperative mortality, morbidity, and length of hospital stay following radical cystectomy. For further sensitivity analysis, propensity score matching was used to yield a total of 1387 matched pairs and primary outcomes were also assessed in the matched cohort.</p><p><strong>Results: </strong>Compared with patients with a MELD < 10, those with MELD ⩾ 10 had significantly higher rates of mortality [odds ratio (OR) = 1.71, <i>p =</i> 0.004], major complications (OR = 1.42, <i>p <</i> 0.001), and prolonged hospital stay (OR = 1.29, <i>p <</i> 0.001) on multivariate analysis. Following risk-adjustment for race, propensity-matched groups revealed that patients with MELD score ⩾ 10 were significantly associated with higher mortality (OR = 1.85, <i>p =</i> 0.008), major complications (OR = 1.34, <i>p <</i> 0.001), yet similar length of hospital stay (OR = 1.17, <i>p =</i> 0.072).</p><p><strong>Conclusion: </strong>MELD score ⩾ 10 is associated with higher mortality and morbidity in patients undergoing radical cystectomy compared with lower MELD scores. Risk-stratification using MELD score may assist clinicians in identifying high-risk patients to provide adequate preoperative counseling, optimize perioperative conditions, and even consider nonsurgical alternatives.</p>\",\"PeriodicalId\":2,\"journal\":{\"name\":\"ACS Applied Bio Materials\",\"volume\":\" \",\"pages\":\"17562872221135944\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2022-11-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/96/8f/10.1177_17562872221135944.PMC9669693.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACS Applied Bio Materials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562872221135944\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MATERIALS SCIENCE, BIOMATERIALS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Bio Materials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562872221135944","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MATERIALS SCIENCE, BIOMATERIALS","Score":null,"Total":0}
Preoperative MELD score predicts mortality and adverse outcomes following radical cystectomy: analysis of American College of Surgeons National Surgical Quality Improvement Program.
Background: The model for end-stage liver disease (MELD) has been widely used to predict the mortality and morbidity of various surgical procedures.
Objectives: We aimed to correlate a high preoperative MELD score with adverse 30-day postoperative complications following radical cystectomy.
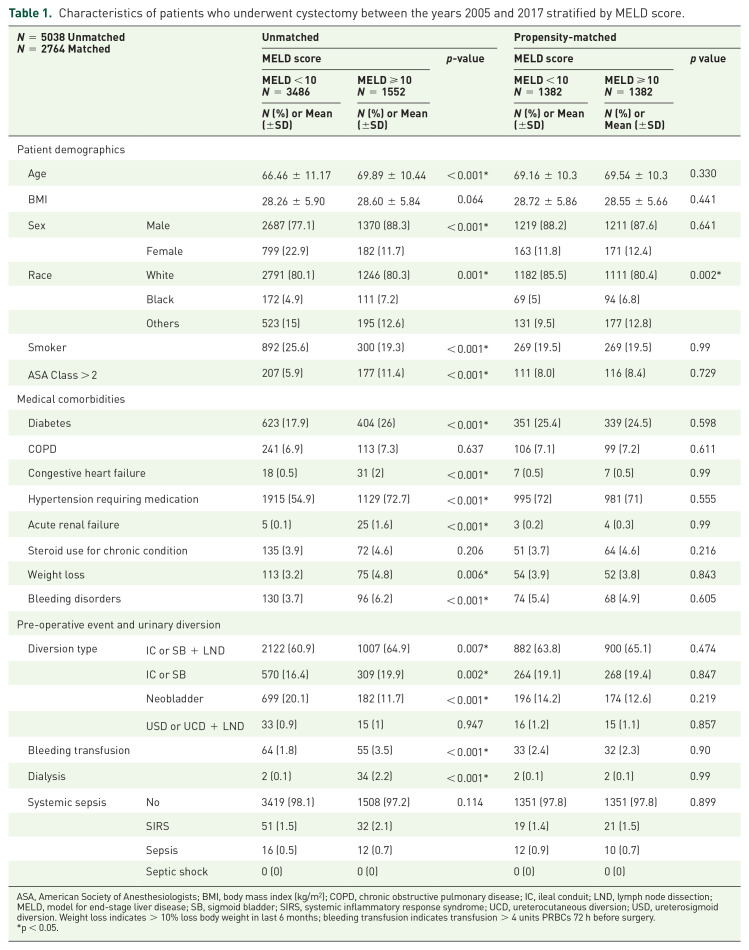
Design and methods: Patients who underwent elective, non-emergency radical cystectomy were identified from the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005 to 2017. Patients were categorized according to a calculated MELD score. The primary outcomes of this study were 30-day postoperative mortality, morbidity, and length of hospital stay following radical cystectomy. For further sensitivity analysis, propensity score matching was used to yield a total of 1387 matched pairs and primary outcomes were also assessed in the matched cohort.
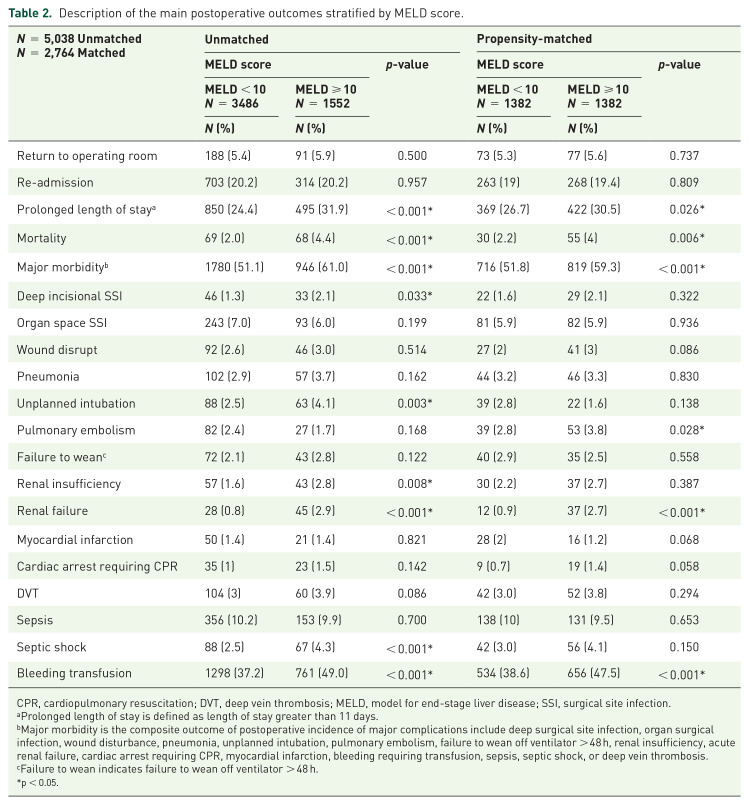
Results: Compared with patients with a MELD < 10, those with MELD ⩾ 10 had significantly higher rates of mortality [odds ratio (OR) = 1.71, p = 0.004], major complications (OR = 1.42, p < 0.001), and prolonged hospital stay (OR = 1.29, p < 0.001) on multivariate analysis. Following risk-adjustment for race, propensity-matched groups revealed that patients with MELD score ⩾ 10 were significantly associated with higher mortality (OR = 1.85, p = 0.008), major complications (OR = 1.34, p < 0.001), yet similar length of hospital stay (OR = 1.17, p = 0.072).
Conclusion: MELD score ⩾ 10 is associated with higher mortality and morbidity in patients undergoing radical cystectomy compared with lower MELD scores. Risk-stratification using MELD score may assist clinicians in identifying high-risk patients to provide adequate preoperative counseling, optimize perioperative conditions, and even consider nonsurgical alternatives.
期刊介绍:
ACS Applied Bio Materials is an interdisciplinary journal publishing original research covering all aspects of biomaterials and biointerfaces including and beyond the traditional biosensing, biomedical and therapeutic applications.
The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrates knowledge in the areas of materials, engineering, physics, bioscience, and chemistry into important bio applications. The journal is specifically interested in work that addresses the relationship between structure and function and assesses the stability and degradation of materials under relevant environmental and biological conditions.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
