{"title":"蛛网膜下腔出血并发骨化性蛛网膜炎1例。","authors":"Yoshitaka Nagashima, Yusuke Nishimura, Hiroshi Ito, Tomoya Nishii, Takahiro Oyama, Ryuta Saito","doi":"10.2176/jns-nmc.2022-0036","DOIUrl":null,"url":null,"abstract":"<p><p>Arachnoiditis ossificans (AO) is a rare disease, wherein ossified lesions in the subarachnoid space obstruct the flow of spinal fluid or compress the spinal cord, thereby causing myelopathy. Here we describe a rare case of AO and discuss the diagnosis and treatment strategies for this disease. A 66-year-old man with a history of subarachnoid hemorrhage presented with gait disturbance and dysuria for 7 months. Spinal magnetic resonance imaging and computed tomography (CT) myelography showed syringomyelia at the T5-T8 level and dorsally tethered spinal cord at the T8-T10 level. Preoperative noncontrast CT was not performed. The patient was diagnosed with adhesive arachnoiditis and underwent arachnoidolysis. However, intraoperative findings showed the presence of ossification lesions on the dorsal surface of the spinal cord, and intraoperative ultrasound (IOU) showed a hyperintense lesion with acoustic shadowing on the dorsal surface of the spinal cord, with limited visibility of the spinal cord. After removal of the lesions, IOU showed untethered and well-decompressed spinal cord and restoration of cerebrospinal fluid pulsation. Based on these findings, the patient was finally diagnosed with AO, which is an extremely rare disease, with an unknown frequency of occurrence. Therefore, all patients with adhesive spinal arachnoiditis require a preoperative noncontrast CT scan to evaluate for ossification lesions. In this case, we were fortunate to be able to treat AO with IOU, which demonstrated specific findings.</p>","PeriodicalId":19260,"journal":{"name":"NMC Case Report Journal","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2022-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/62/3f/2188-4226-9-0295.PMC9534567.pdf","citationCount":"0","resultStr":"{\"title\":\"Diagnosis and Treatment Strategies for Arachnoiditis Ossificans Following Subarachnoid Hemorrhage: A Case Report.\",\"authors\":\"Yoshitaka Nagashima, Yusuke Nishimura, Hiroshi Ito, Tomoya Nishii, Takahiro Oyama, Ryuta Saito\",\"doi\":\"10.2176/jns-nmc.2022-0036\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Arachnoiditis ossificans (AO) is a rare disease, wherein ossified lesions in the subarachnoid space obstruct the flow of spinal fluid or compress the spinal cord, thereby causing myelopathy. Here we describe a rare case of AO and discuss the diagnosis and treatment strategies for this disease. A 66-year-old man with a history of subarachnoid hemorrhage presented with gait disturbance and dysuria for 7 months. Spinal magnetic resonance imaging and computed tomography (CT) myelography showed syringomyelia at the T5-T8 level and dorsally tethered spinal cord at the T8-T10 level. Preoperative noncontrast CT was not performed. The patient was diagnosed with adhesive arachnoiditis and underwent arachnoidolysis. However, intraoperative findings showed the presence of ossification lesions on the dorsal surface of the spinal cord, and intraoperative ultrasound (IOU) showed a hyperintense lesion with acoustic shadowing on the dorsal surface of the spinal cord, with limited visibility of the spinal cord. After removal of the lesions, IOU showed untethered and well-decompressed spinal cord and restoration of cerebrospinal fluid pulsation. Based on these findings, the patient was finally diagnosed with AO, which is an extremely rare disease, with an unknown frequency of occurrence. Therefore, all patients with adhesive spinal arachnoiditis require a preoperative noncontrast CT scan to evaluate for ossification lesions. In this case, we were fortunate to be able to treat AO with IOU, which demonstrated specific findings.</p>\",\"PeriodicalId\":19260,\"journal\":{\"name\":\"NMC Case Report Journal\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-09-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/62/3f/2188-4226-9-0295.PMC9534567.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NMC Case Report Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2176/jns-nmc.2022-0036\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC Case Report Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2022-0036","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Diagnosis and Treatment Strategies for Arachnoiditis Ossificans Following Subarachnoid Hemorrhage: A Case Report.
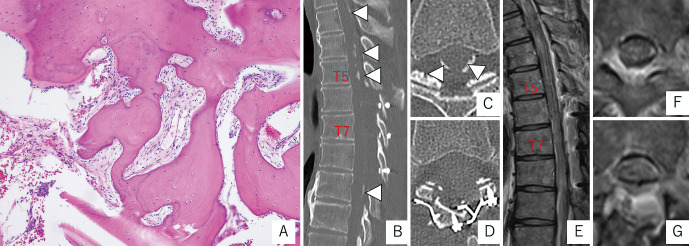
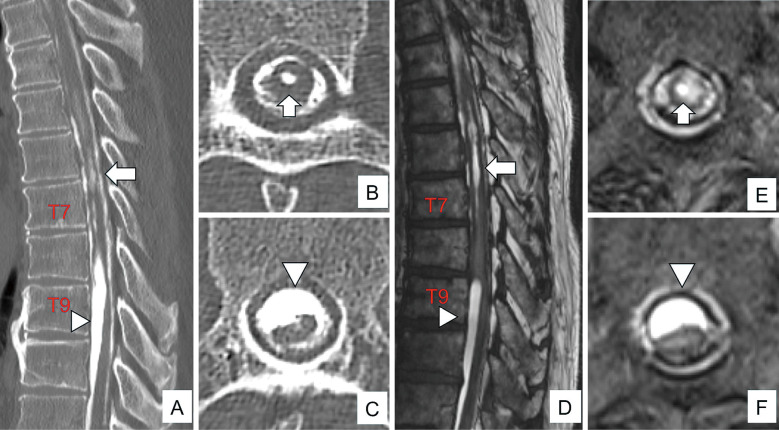
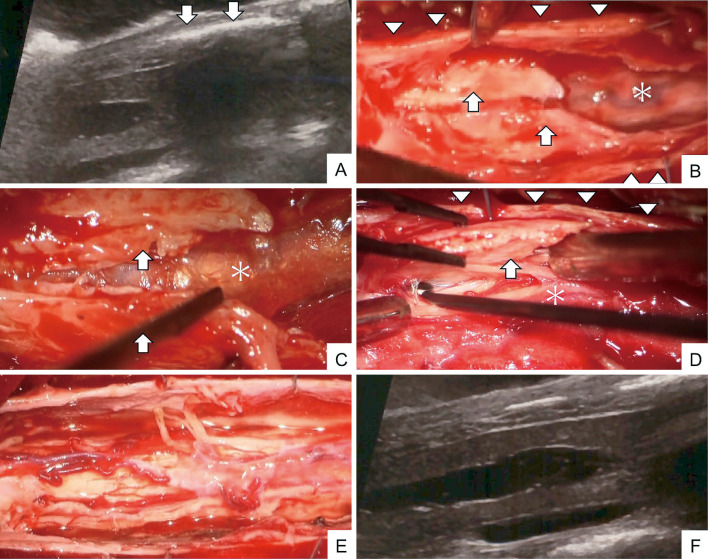
Arachnoiditis ossificans (AO) is a rare disease, wherein ossified lesions in the subarachnoid space obstruct the flow of spinal fluid or compress the spinal cord, thereby causing myelopathy. Here we describe a rare case of AO and discuss the diagnosis and treatment strategies for this disease. A 66-year-old man with a history of subarachnoid hemorrhage presented with gait disturbance and dysuria for 7 months. Spinal magnetic resonance imaging and computed tomography (CT) myelography showed syringomyelia at the T5-T8 level and dorsally tethered spinal cord at the T8-T10 level. Preoperative noncontrast CT was not performed. The patient was diagnosed with adhesive arachnoiditis and underwent arachnoidolysis. However, intraoperative findings showed the presence of ossification lesions on the dorsal surface of the spinal cord, and intraoperative ultrasound (IOU) showed a hyperintense lesion with acoustic shadowing on the dorsal surface of the spinal cord, with limited visibility of the spinal cord. After removal of the lesions, IOU showed untethered and well-decompressed spinal cord and restoration of cerebrospinal fluid pulsation. Based on these findings, the patient was finally diagnosed with AO, which is an extremely rare disease, with an unknown frequency of occurrence. Therefore, all patients with adhesive spinal arachnoiditis require a preoperative noncontrast CT scan to evaluate for ossification lesions. In this case, we were fortunate to be able to treat AO with IOU, which demonstrated specific findings.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
