Praveen Ratanasrimetha , Biruh T. Workeneh , Harish Seethapathy
{"title":"癌症患者的钠钾失调","authors":"Praveen Ratanasrimetha , Biruh T. Workeneh , Harish Seethapathy","doi":"10.1053/j.ackd.2022.01.003","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>Sodium and potassium disorders are pervasive in patients<span><span><span> with cancer. The causes of these abnormalities are wide-ranging, are often primary or second-order consequences of the underlying cancer, and have prognostic implications. The approach to hyponatremia should focus on cancer-related etiologies, such as syndrome of inappropriate </span>antidiuretic hormone, to the exclusion of other causes. </span>Hypernatremia<span><span> in non-iatrogenic forms is generally due to water loss<span> rather than excessive sodium intake. Debilitated or dependent patients with cancer are particularly vulnerable to hypernatremia. </span></span>Hypokalemia<span> can occur in patients with cancer due to gastrointestinal disturbances, resulting from decreased intake or increased losses. Renal losses can occur as a result of excessive </span></span></span></span>mineralocorticoid<span><span> secretion or therapy-related nephrotoxicity. The approach to </span>hyperkalemia should be informed by historical and laboratory clues, and pseudohyperkalemia is particularly common in patients with </span></span>hematological cancers<span><span>. Hyperkalemia can be seen in primary or metastatic disease<span> that interrupts the adrenal axis. It can also develop as a consequence of immunotherapy<span>, which can cause adrenalitis or hypophysitis. </span></span></span>Tumor lysis syndrome (TLS) is defined by the development of hyperkalemia and is a medical emergency. Awareness of the electrolyte abnormalities that can befall patients with cancer is vital for its prompt recognition and management.</span></p></div>","PeriodicalId":7221,"journal":{"name":"Advances in chronic kidney disease","volume":"29 2","pages":"Pages 171-179.e1"},"PeriodicalIF":2.3000,"publicationDate":"2022-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"2","resultStr":"{\"title\":\"Sodium and Potassium Dysregulation in the Patient With Cancer\",\"authors\":\"Praveen Ratanasrimetha , Biruh T. Workeneh , Harish Seethapathy\",\"doi\":\"10.1053/j.ackd.2022.01.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span><span>Sodium and potassium disorders are pervasive in patients<span><span><span> with cancer. The causes of these abnormalities are wide-ranging, are often primary or second-order consequences of the underlying cancer, and have prognostic implications. The approach to hyponatremia should focus on cancer-related etiologies, such as syndrome of inappropriate </span>antidiuretic hormone, to the exclusion of other causes. </span>Hypernatremia<span><span> in non-iatrogenic forms is generally due to water loss<span> rather than excessive sodium intake. Debilitated or dependent patients with cancer are particularly vulnerable to hypernatremia. </span></span>Hypokalemia<span> can occur in patients with cancer due to gastrointestinal disturbances, resulting from decreased intake or increased losses. Renal losses can occur as a result of excessive </span></span></span></span>mineralocorticoid<span><span> secretion or therapy-related nephrotoxicity. The approach to </span>hyperkalemia should be informed by historical and laboratory clues, and pseudohyperkalemia is particularly common in patients with </span></span>hematological cancers<span><span>. Hyperkalemia can be seen in primary or metastatic disease<span> that interrupts the adrenal axis. It can also develop as a consequence of immunotherapy<span>, which can cause adrenalitis or hypophysitis. </span></span></span>Tumor lysis syndrome (TLS) is defined by the development of hyperkalemia and is a medical emergency. Awareness of the electrolyte abnormalities that can befall patients with cancer is vital for its prompt recognition and management.</span></p></div>\",\"PeriodicalId\":7221,\"journal\":{\"name\":\"Advances in chronic kidney disease\",\"volume\":\"29 2\",\"pages\":\"Pages 171-179.e1\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2022-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in chronic kidney disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1548559522000039\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in chronic kidney disease","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1548559522000039","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Sodium and Potassium Dysregulation in the Patient With Cancer
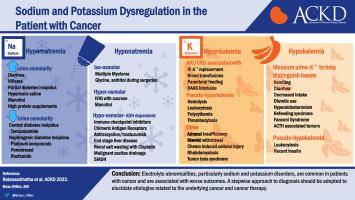
Sodium and potassium disorders are pervasive in patients with cancer. The causes of these abnormalities are wide-ranging, are often primary or second-order consequences of the underlying cancer, and have prognostic implications. The approach to hyponatremia should focus on cancer-related etiologies, such as syndrome of inappropriate antidiuretic hormone, to the exclusion of other causes. Hypernatremia in non-iatrogenic forms is generally due to water loss rather than excessive sodium intake. Debilitated or dependent patients with cancer are particularly vulnerable to hypernatremia. Hypokalemia can occur in patients with cancer due to gastrointestinal disturbances, resulting from decreased intake or increased losses. Renal losses can occur as a result of excessive mineralocorticoid secretion or therapy-related nephrotoxicity. The approach to hyperkalemia should be informed by historical and laboratory clues, and pseudohyperkalemia is particularly common in patients with hematological cancers. Hyperkalemia can be seen in primary or metastatic disease that interrupts the adrenal axis. It can also develop as a consequence of immunotherapy, which can cause adrenalitis or hypophysitis. Tumor lysis syndrome (TLS) is defined by the development of hyperkalemia and is a medical emergency. Awareness of the electrolyte abnormalities that can befall patients with cancer is vital for its prompt recognition and management.
期刊介绍:
The purpose of Advances Chronic Kidney Disease is to provide in-depth, scholarly review articles about the care and management of persons with early kidney disease and kidney failure, as well as those at risk for kidney disease. Emphasis is on articles related to the early identification of kidney disease; prevention or delay in progression of kidney disease




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
