Janina Paula T. Sy-Go , Sandra M. Herrmann , Surya V. Seshan
{"title":"单克隆伽玛病相关肾病","authors":"Janina Paula T. Sy-Go , Sandra M. Herrmann , Surya V. Seshan","doi":"10.1053/j.ackd.2022.01.004","DOIUrl":null,"url":null,"abstract":"<div><p><span><span><span>Monoclonal gammopathies occur secondary to a broad range of clonal </span>B lymphocyte or plasma cell disorders, producing either whole or truncated </span>monoclonal immunoglobulins<span><span><span><span>. The kidneys are often affected by these monoclonal proteins, and, although not mutually exclusive, can involve the glomeruli, tubules, </span>interstitium, and </span>vasculature<span>. The nephrotoxic potential of these monoclonal proteins is dependent on a variety of physicochemical characteristics that are responsible for the diverse clinicopathologic manifestations, including glomerular diseases<span> with organized deposits, glomerular diseases with granular deposits, and other lesions, such as C3 glomerulopathy and thrombotic microangiopathy with unique pathophysiologic features. The diseases that involve primarily the tubulointerstitial and vascular compartments are light chain cast </span></span></span>nephropathy<span>, light chain proximal tubulopathy, crystal-storing </span></span></span>histiocytosis<span>, and crystalglobulin-induced nephropathy with distinct acute and chronic clinicopathologic features. The diagnosis of a monoclonal gammopathy–related kidney disease is established by identification of an underlying active or more commonly, low-grade hematologic malignancy<span><span>, serologic evidence of a monoclonal gammopathy when detectable, and most importantly, monoclonal protein–induced pathologic lesions seen in a kidney biopsy, confirming the association with the monoclonal protein. Establishing a diagnosis may be challenging at times, particularly in the absence of an overt hematologic malignancy, with or without monoclonal gammopathy, such as </span>proliferative glomerulonephritis<span> with monoclonal immunoglobulin deposits. Overall, the treatment is directed against the underlying hematologic disorder and the potential source of the monoclonal protein.</span></span></span></p></div>","PeriodicalId":7221,"journal":{"name":"Advances in chronic kidney disease","volume":"29 2","pages":"Pages 86-102.e1"},"PeriodicalIF":2.3000,"publicationDate":"2022-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"1","resultStr":"{\"title\":\"Monoclonal Gammopathy–Related Kidney Diseases\",\"authors\":\"Janina Paula T. Sy-Go , Sandra M. Herrmann , Surya V. Seshan\",\"doi\":\"10.1053/j.ackd.2022.01.004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span><span><span>Monoclonal gammopathies occur secondary to a broad range of clonal </span>B lymphocyte or plasma cell disorders, producing either whole or truncated </span>monoclonal immunoglobulins<span><span><span><span>. The kidneys are often affected by these monoclonal proteins, and, although not mutually exclusive, can involve the glomeruli, tubules, </span>interstitium, and </span>vasculature<span>. The nephrotoxic potential of these monoclonal proteins is dependent on a variety of physicochemical characteristics that are responsible for the diverse clinicopathologic manifestations, including glomerular diseases<span> with organized deposits, glomerular diseases with granular deposits, and other lesions, such as C3 glomerulopathy and thrombotic microangiopathy with unique pathophysiologic features. The diseases that involve primarily the tubulointerstitial and vascular compartments are light chain cast </span></span></span>nephropathy<span>, light chain proximal tubulopathy, crystal-storing </span></span></span>histiocytosis<span>, and crystalglobulin-induced nephropathy with distinct acute and chronic clinicopathologic features. The diagnosis of a monoclonal gammopathy–related kidney disease is established by identification of an underlying active or more commonly, low-grade hematologic malignancy<span><span>, serologic evidence of a monoclonal gammopathy when detectable, and most importantly, monoclonal protein–induced pathologic lesions seen in a kidney biopsy, confirming the association with the monoclonal protein. Establishing a diagnosis may be challenging at times, particularly in the absence of an overt hematologic malignancy, with or without monoclonal gammopathy, such as </span>proliferative glomerulonephritis<span> with monoclonal immunoglobulin deposits. Overall, the treatment is directed against the underlying hematologic disorder and the potential source of the monoclonal protein.</span></span></span></p></div>\",\"PeriodicalId\":7221,\"journal\":{\"name\":\"Advances in chronic kidney disease\",\"volume\":\"29 2\",\"pages\":\"Pages 86-102.e1\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2022-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in chronic kidney disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1548559522000027\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in chronic kidney disease","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1548559522000027","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
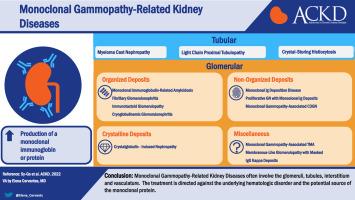
Monoclonal gammopathies occur secondary to a broad range of clonal B lymphocyte or plasma cell disorders, producing either whole or truncated monoclonal immunoglobulins. The kidneys are often affected by these monoclonal proteins, and, although not mutually exclusive, can involve the glomeruli, tubules, interstitium, and vasculature. The nephrotoxic potential of these monoclonal proteins is dependent on a variety of physicochemical characteristics that are responsible for the diverse clinicopathologic manifestations, including glomerular diseases with organized deposits, glomerular diseases with granular deposits, and other lesions, such as C3 glomerulopathy and thrombotic microangiopathy with unique pathophysiologic features. The diseases that involve primarily the tubulointerstitial and vascular compartments are light chain cast nephropathy, light chain proximal tubulopathy, crystal-storing histiocytosis, and crystalglobulin-induced nephropathy with distinct acute and chronic clinicopathologic features. The diagnosis of a monoclonal gammopathy–related kidney disease is established by identification of an underlying active or more commonly, low-grade hematologic malignancy, serologic evidence of a monoclonal gammopathy when detectable, and most importantly, monoclonal protein–induced pathologic lesions seen in a kidney biopsy, confirming the association with the monoclonal protein. Establishing a diagnosis may be challenging at times, particularly in the absence of an overt hematologic malignancy, with or without monoclonal gammopathy, such as proliferative glomerulonephritis with monoclonal immunoglobulin deposits. Overall, the treatment is directed against the underlying hematologic disorder and the potential source of the monoclonal protein.
期刊介绍:
The purpose of Advances Chronic Kidney Disease is to provide in-depth, scholarly review articles about the care and management of persons with early kidney disease and kidney failure, as well as those at risk for kidney disease. Emphasis is on articles related to the early identification of kidney disease; prevention or delay in progression of kidney disease



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
