Seung Jae Lee, In Seok Choi, Ju Ik Moon, Dae Sung Yoon, Won Jun Choi, Sang Eok Lee, Nak Song Sung, Seong Uk Kwon, In Eui Bae, Seung Jae Roh, Sung Gon Kim
{"title":"急性胆囊炎复杂腹腔镜胆囊切除术后最佳引流管理:倾向匹配的比较研究。","authors":"Seung Jae Lee, In Seok Choi, Ju Ik Moon, Dae Sung Yoon, Won Jun Choi, Sang Eok Lee, Nak Song Sung, Seong Uk Kwon, In Eui Bae, Seung Jae Roh, Sung Gon Kim","doi":"10.7602/jmis.2022.25.2.63","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study was performed to investigate the effect of drain placement on complicated laparoscopic cholecystectomy (cLC) for acute cholecystitis (AC).</p><p><strong>Methods: </strong>This single-center retrospective study reviewed patients with AC who underwent cLC between January 2010 and December 2020. cLC was defined as open conversion, subtotal cholecystectomy, adjacent organ injury during surgery, operation time of ≥90 minutes, or estimated blood loss of ≥100 mL. One-to-one propensity score matching was performed to compare the surgical outcomes between patients with and without drain on cLC.</p><p><strong>Results: </strong>A total of 216 patients (mean age, 65.8 years; 75 female patients [34.7%]) underwent cLC, and 126 (58.3%) underwent intraoperative abdominal drainage. In the propensity score-matched cohort (61 patients in each group), early drain removal (≤postoperative day 3) was performed in 42 patients (68.9%). The overall rate of surgical site infection (SSI) was 10.7%. Late drain removal demonstrated significantly worse surgical outcomes than no drain placement and early drain removal for overall complications (13.1% vs. 21.4% vs. 47.4%, <i>p</i> = 0.006), postoperative hospital stay (3.8 days vs. 4.4 days vs. 12.7 days, <i>p</i> < 0.001), and SSI (4.9% vs. 11.9% vs. 31.6%, <i>p</i> = 0.006). In the multivariate analysis, late drain removal was the most significant risk factor for organ space SSI.</p><p><strong>Conclusion: </strong>This study demonstrated that drain placement is not routinely recommended, even after cLC for AC. When placing a drain, early drain removal is recommended because late drain removal is associated with a higher risk of organ space SSI.</p>","PeriodicalId":73832,"journal":{"name":"Journal of minimally invasive surgery","volume":"25 2","pages":"63-72"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/91/db/jmis-25-2-63.PMC9218398.pdf","citationCount":"1","resultStr":"{\"title\":\"Optimal drain management following complicated laparoscopic cholecystectomy for acute cholecystitis: a propensity-matched comparative study.\",\"authors\":\"Seung Jae Lee, In Seok Choi, Ju Ik Moon, Dae Sung Yoon, Won Jun Choi, Sang Eok Lee, Nak Song Sung, Seong Uk Kwon, In Eui Bae, Seung Jae Roh, Sung Gon Kim\",\"doi\":\"10.7602/jmis.2022.25.2.63\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>This study was performed to investigate the effect of drain placement on complicated laparoscopic cholecystectomy (cLC) for acute cholecystitis (AC).</p><p><strong>Methods: </strong>This single-center retrospective study reviewed patients with AC who underwent cLC between January 2010 and December 2020. cLC was defined as open conversion, subtotal cholecystectomy, adjacent organ injury during surgery, operation time of ≥90 minutes, or estimated blood loss of ≥100 mL. One-to-one propensity score matching was performed to compare the surgical outcomes between patients with and without drain on cLC.</p><p><strong>Results: </strong>A total of 216 patients (mean age, 65.8 years; 75 female patients [34.7%]) underwent cLC, and 126 (58.3%) underwent intraoperative abdominal drainage. In the propensity score-matched cohort (61 patients in each group), early drain removal (≤postoperative day 3) was performed in 42 patients (68.9%). The overall rate of surgical site infection (SSI) was 10.7%. Late drain removal demonstrated significantly worse surgical outcomes than no drain placement and early drain removal for overall complications (13.1% vs. 21.4% vs. 47.4%, <i>p</i> = 0.006), postoperative hospital stay (3.8 days vs. 4.4 days vs. 12.7 days, <i>p</i> < 0.001), and SSI (4.9% vs. 11.9% vs. 31.6%, <i>p</i> = 0.006). In the multivariate analysis, late drain removal was the most significant risk factor for organ space SSI.</p><p><strong>Conclusion: </strong>This study demonstrated that drain placement is not routinely recommended, even after cLC for AC. When placing a drain, early drain removal is recommended because late drain removal is associated with a higher risk of organ space SSI.</p>\",\"PeriodicalId\":73832,\"journal\":{\"name\":\"Journal of minimally invasive surgery\",\"volume\":\"25 2\",\"pages\":\"63-72\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-06-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/91/db/jmis-25-2-63.PMC9218398.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of minimally invasive surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7602/jmis.2022.25.2.63\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of minimally invasive surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7602/jmis.2022.25.2.63","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
目的:探讨急性胆囊炎(AC)并发腹腔镜胆囊切除术(cLC)引流管放置的效果。方法:这项单中心回顾性研究回顾了2010年1月至2020年12月期间接受cLC治疗的AC患者。cLC定义为开腹转换、胆囊次全切除术、术中邻近器官损伤、手术时间≥90分钟或估计失血量≥100 mL。采用一对一倾向评分匹配来比较cLC患者有引流和没有引流的手术结果。结果:共216例患者,平均年龄65.8岁;女性75例(34.7%)行小细胞肺癌,126例(58.3%)行术中腹腔引流。在倾向评分匹配的队列中(每组61例),42例患者(68.9%)进行了早期引流术(≤术后第3天)。手术部位感染(SSI)总发生率为10.7%。在总体并发症、术后住院时间(3.8天vs. 4.4天vs. 12.7天,p < 0.001)和SSI (4.9% vs. 11.9% vs. 31.6%, p = 0.006)方面,晚置引流管的手术结果明显差于未置引流管和早期引流管的手术结果(13.1% vs. 21.4% vs. 47.4%, p = 0.006)。在多因素分析中,晚期引流术是器官间隙SSI最重要的危险因素。结论:本研究表明,即使在cLC为AC后,也不推荐放置引流管。当放置引流管时,建议早期摘除引流管,因为晚期摘除引流管会增加器官间隙SSI的风险。
Optimal drain management following complicated laparoscopic cholecystectomy for acute cholecystitis: a propensity-matched comparative study.
Purpose: This study was performed to investigate the effect of drain placement on complicated laparoscopic cholecystectomy (cLC) for acute cholecystitis (AC).
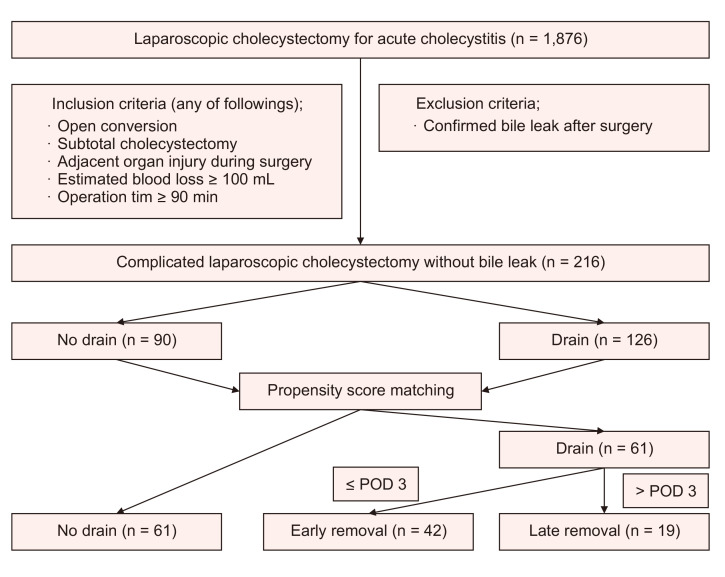
Methods: This single-center retrospective study reviewed patients with AC who underwent cLC between January 2010 and December 2020. cLC was defined as open conversion, subtotal cholecystectomy, adjacent organ injury during surgery, operation time of ≥90 minutes, or estimated blood loss of ≥100 mL. One-to-one propensity score matching was performed to compare the surgical outcomes between patients with and without drain on cLC.
Results: A total of 216 patients (mean age, 65.8 years; 75 female patients [34.7%]) underwent cLC, and 126 (58.3%) underwent intraoperative abdominal drainage. In the propensity score-matched cohort (61 patients in each group), early drain removal (≤postoperative day 3) was performed in 42 patients (68.9%). The overall rate of surgical site infection (SSI) was 10.7%. Late drain removal demonstrated significantly worse surgical outcomes than no drain placement and early drain removal for overall complications (13.1% vs. 21.4% vs. 47.4%, p = 0.006), postoperative hospital stay (3.8 days vs. 4.4 days vs. 12.7 days, p < 0.001), and SSI (4.9% vs. 11.9% vs. 31.6%, p = 0.006). In the multivariate analysis, late drain removal was the most significant risk factor for organ space SSI.
Conclusion: This study demonstrated that drain placement is not routinely recommended, even after cLC for AC. When placing a drain, early drain removal is recommended because late drain removal is associated with a higher risk of organ space SSI.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
