Ramy M. Hanna , Kammi Henriksen , Kamyar Kalantar-Zadeh , Antoney Ferrey , Richard Burwick , Kenar D. Jhaveri
{"title":"血栓性微血管病综合征——共同点和不同的前沿","authors":"Ramy M. Hanna , Kammi Henriksen , Kamyar Kalantar-Zadeh , Antoney Ferrey , Richard Burwick , Kenar D. Jhaveri","doi":"10.1053/j.ackd.2021.11.006","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>Thrombotic microangiopathies (TMAs) have in common a terminal phenotype of microangiopathic </span>hemolytic anemia with end-organ dysfunction. Thrombotic thrombocytopenic purpura results from </span>von Willebrand factor<span><span><span><span> multimerization, Shiga toxin–mediated hemolytic uremic syndrome causes toxin-induced </span>endothelial dysfunction<span><span>, while atypical hemolytic uremic syndrome results from complement system dysregulation. Drug-induced TMA, rheumatological disease–induced TMA, and renal-limited TMA exist in an intermediate space that represents secondary complement activation and may overlap with atypical hemolytic uremic syndrome clinically. The existence of TMA without microangiopathic hemolytic features, renal-limited TMA, represents an undiscovered syndrome that responds incompletely and inconsistently to complement blockade. Hematopoietic stem cell transplant-TMA represents another more resistant form of TMA with different therapeutic needs and clinical course. It has become apparent that TMA syndromes are an emerging field in </span>nephrology, </span></span>rheumatology, and </span>hematology. Much work remains in genetics, molecular biology, and therapeutics to unravel the puzzle of the relationships and distinctions apparent between the different subclasses of TMA syndromes.</span></p></div>","PeriodicalId":7221,"journal":{"name":"Advances in chronic kidney disease","volume":"29 2","pages":"Pages 149-160.e1"},"PeriodicalIF":2.3000,"publicationDate":"2022-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"4","resultStr":"{\"title\":\"Thrombotic Microangiopathy Syndromes—Common Ground and Distinct Frontiers\",\"authors\":\"Ramy M. Hanna , Kammi Henriksen , Kamyar Kalantar-Zadeh , Antoney Ferrey , Richard Burwick , Kenar D. Jhaveri\",\"doi\":\"10.1053/j.ackd.2021.11.006\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span><span>Thrombotic microangiopathies (TMAs) have in common a terminal phenotype of microangiopathic </span>hemolytic anemia with end-organ dysfunction. Thrombotic thrombocytopenic purpura results from </span>von Willebrand factor<span><span><span><span> multimerization, Shiga toxin–mediated hemolytic uremic syndrome causes toxin-induced </span>endothelial dysfunction<span><span>, while atypical hemolytic uremic syndrome results from complement system dysregulation. Drug-induced TMA, rheumatological disease–induced TMA, and renal-limited TMA exist in an intermediate space that represents secondary complement activation and may overlap with atypical hemolytic uremic syndrome clinically. The existence of TMA without microangiopathic hemolytic features, renal-limited TMA, represents an undiscovered syndrome that responds incompletely and inconsistently to complement blockade. Hematopoietic stem cell transplant-TMA represents another more resistant form of TMA with different therapeutic needs and clinical course. It has become apparent that TMA syndromes are an emerging field in </span>nephrology, </span></span>rheumatology, and </span>hematology. Much work remains in genetics, molecular biology, and therapeutics to unravel the puzzle of the relationships and distinctions apparent between the different subclasses of TMA syndromes.</span></p></div>\",\"PeriodicalId\":7221,\"journal\":{\"name\":\"Advances in chronic kidney disease\",\"volume\":\"29 2\",\"pages\":\"Pages 149-160.e1\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2022-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in chronic kidney disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1548559521001488\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in chronic kidney disease","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1548559521001488","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
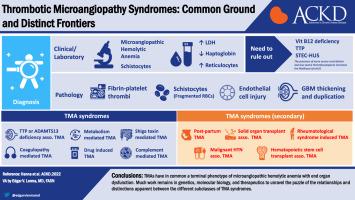
Thrombotic Microangiopathy Syndromes—Common Ground and Distinct Frontiers
Thrombotic microangiopathies (TMAs) have in common a terminal phenotype of microangiopathic hemolytic anemia with end-organ dysfunction. Thrombotic thrombocytopenic purpura results from von Willebrand factor multimerization, Shiga toxin–mediated hemolytic uremic syndrome causes toxin-induced endothelial dysfunction, while atypical hemolytic uremic syndrome results from complement system dysregulation. Drug-induced TMA, rheumatological disease–induced TMA, and renal-limited TMA exist in an intermediate space that represents secondary complement activation and may overlap with atypical hemolytic uremic syndrome clinically. The existence of TMA without microangiopathic hemolytic features, renal-limited TMA, represents an undiscovered syndrome that responds incompletely and inconsistently to complement blockade. Hematopoietic stem cell transplant-TMA represents another more resistant form of TMA with different therapeutic needs and clinical course. It has become apparent that TMA syndromes are an emerging field in nephrology, rheumatology, and hematology. Much work remains in genetics, molecular biology, and therapeutics to unravel the puzzle of the relationships and distinctions apparent between the different subclasses of TMA syndromes.
期刊介绍:
The purpose of Advances Chronic Kidney Disease is to provide in-depth, scholarly review articles about the care and management of persons with early kidney disease and kidney failure, as well as those at risk for kidney disease. Emphasis is on articles related to the early identification of kidney disease; prevention or delay in progression of kidney disease




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
