{"title":"临床表现:抗合成酶综合征伴肝结节性再生增生。","authors":"Yi-Ning Yen, Hsien-Tzung Liao","doi":"10.1002/acr2.11491","DOIUrl":null,"url":null,"abstract":"in (1 anti – glycyl – transfer RNA synthetase antibody, proximal girdle high serum level of creatine phosphokinase, phenomenon of fi ngers, interstitial the progres-sive distention and bilateral lower extremities edematous change. A laboratory examination revealed elevated alanine aminotransferase (368 U/l) and aspartate aminotransferase (192 U/l) levels but a normal alpha-fetoprotein level (1.04 ng/ml). Abdominal computed tomography ( A : axial section, venous phase, slice thickness 5 mm; B : coronal reformatted section, venous phase, slice thickness 5 mm) numerous widespread hepatic enhancing nodules and massive ascites without any lymphadenopathy in the para-aortic retroperitoneum or pelvic cavity. hepatocellular carcinoma or liver metastasis was suspected. a liver biopsy showed sinusoidal dilatation but no malignant cell, signi fi cant lobular or portal in fl ammation, or advanced fi brosis by Masson trichrome Plasma not by a Mum1 stain. Iron stain and Congo red stain results were also negative. A reticulin stain of the ( thickened hepatic cell plates (arrows) compressing adjacent hepatocytes","PeriodicalId":7084,"journal":{"name":"ACR Open Rheumatology","volume":" ","pages":"933-934"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/21/f4/ACR2-4-933.PMC9661828.pdf","citationCount":"0","resultStr":"{\"title\":\"Clinical Images: Liver nodular regenerative hyperplasia in antisynthetase syndrome.\",\"authors\":\"Yi-Ning Yen, Hsien-Tzung Liao\",\"doi\":\"10.1002/acr2.11491\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"in (1 anti – glycyl – transfer RNA synthetase antibody, proximal girdle high serum level of creatine phosphokinase, phenomenon of fi ngers, interstitial the progres-sive distention and bilateral lower extremities edematous change. A laboratory examination revealed elevated alanine aminotransferase (368 U/l) and aspartate aminotransferase (192 U/l) levels but a normal alpha-fetoprotein level (1.04 ng/ml). Abdominal computed tomography ( A : axial section, venous phase, slice thickness 5 mm; B : coronal reformatted section, venous phase, slice thickness 5 mm) numerous widespread hepatic enhancing nodules and massive ascites without any lymphadenopathy in the para-aortic retroperitoneum or pelvic cavity. hepatocellular carcinoma or liver metastasis was suspected. a liver biopsy showed sinusoidal dilatation but no malignant cell, signi fi cant lobular or portal in fl ammation, or advanced fi brosis by Masson trichrome Plasma not by a Mum1 stain. Iron stain and Congo red stain results were also negative. A reticulin stain of the ( thickened hepatic cell plates (arrows) compressing adjacent hepatocytes\",\"PeriodicalId\":7084,\"journal\":{\"name\":\"ACR Open Rheumatology\",\"volume\":\" \",\"pages\":\"933-934\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/21/f4/ACR2-4-933.PMC9661828.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACR Open Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/acr2.11491\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/8/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR Open Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.11491","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/8/2 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Clinical Images: Liver nodular regenerative hyperplasia in antisynthetase syndrome.
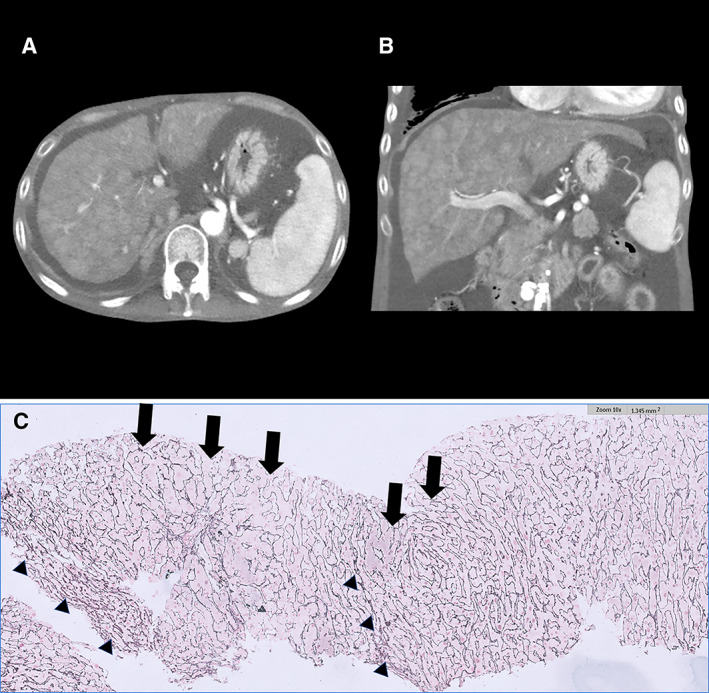
in (1 anti – glycyl – transfer RNA synthetase antibody, proximal girdle high serum level of creatine phosphokinase, phenomenon of fi ngers, interstitial the progres-sive distention and bilateral lower extremities edematous change. A laboratory examination revealed elevated alanine aminotransferase (368 U/l) and aspartate aminotransferase (192 U/l) levels but a normal alpha-fetoprotein level (1.04 ng/ml). Abdominal computed tomography ( A : axial section, venous phase, slice thickness 5 mm; B : coronal reformatted section, venous phase, slice thickness 5 mm) numerous widespread hepatic enhancing nodules and massive ascites without any lymphadenopathy in the para-aortic retroperitoneum or pelvic cavity. hepatocellular carcinoma or liver metastasis was suspected. a liver biopsy showed sinusoidal dilatation but no malignant cell, signi fi cant lobular or portal in fl ammation, or advanced fi brosis by Masson trichrome Plasma not by a Mum1 stain. Iron stain and Congo red stain results were also negative. A reticulin stain of the ( thickened hepatic cell plates (arrows) compressing adjacent hepatocytes



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
