Soon Yaw Walter Wong, Fen Li Stephanie Ler, Rehena Sultana, Hamid Rahmatullah Bin Abd Razak
{"title":"亚洲人进行全膝关节置换术后预防静脉血栓栓塞的最佳方法是什么?系统综述和网络荟萃分析。","authors":"Soon Yaw Walter Wong, Fen Li Stephanie Ler, Rehena Sultana, Hamid Rahmatullah Bin Abd Razak","doi":"10.1186/s43019-022-00166-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Asians have a low venous thromboembolism (VTE) incidence following total knee arthroplasty (TKA). This systematic review and network meta-analysis was conducted to evaluate the best prophylaxis against VTE in Asians following total knee arthroplasty in current literature.</p><p><strong>Materials and methods: </strong>A systematic search of PubMed, Embase and CINAHL was conducted in adherence with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Prophylaxis types were separated into low-molecular-weight heparin (LMWH), novel oral anti-coagulants (NOAC), mechanical-only prophylaxis (MOP) and no prophylaxis (NP). The primary outcome was VTE incidence, grouped according to diagnosis modality (ultrasound, venography, clinical). The secondary outcome was bleeding incidence, grouped into minor and major bleeding.</p><p><strong>Results: </strong>Fourteen eligible articles, totalling 4259 patients, were pooled with the following significant results: NOACs had lower venography-diagnosed VTE incidence than LMWH (12.77%, p = 0.02) and NP (20.64, p < 0.001). MOP had lower venography-diagnosed VTE incidence than LMWH (23.72%, p < 0.001), NOACs (10.95%, p < 0.001) and NP (31.59%, p < 0.001) but, interestingly, a statistically higher ultrasound-diagnosed VTE incidence than LMWH (6.56%, p = 0.024) and NP (4.88%, p = 0.026). No significant differences were observed between prophylaxis types for symptomatic VTE, pulmonary embolism (PE) or death. LMWH and NOACs had a higher minor bleeding incidence than NP (11.71%, p < 0.001 and 6.33%, p < 0.02, respectively). No significant differences were observed between prophylaxis types for major bleeding incidence.</p><p><strong>Conclusion: </strong>NOACs are a superior form of chemoprophylaxis, compared with LMWH, in reducing venography-diagnosed VTE incidence with no added bleeding incidence. However, routine chemoprophylaxis may not be required as LMWH and NOACs do not appear to reduce symptomatic VTE incidence compared with MOP and NP with an increased minor bleeding incidence. Mechanical prophylaxis in the form of graduated compression stockings or intermittent pneumatic compression should be routinely considered with significantly lower rates of venography-diagnosed VTE compared with NP. On the basis of current evidence, we recommend an individualised approach to select the most appropriate prophylaxis type.</p>","PeriodicalId":4,"journal":{"name":"ACS Applied Energy Materials","volume":" ","pages":"37"},"PeriodicalIF":5.5000,"publicationDate":"2022-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9375282/pdf/","citationCount":"0","resultStr":"{\"title\":\"What is the best prophylaxis against venous thromboembolism in Asians following total knee arthroplasty? A systematic review and network meta-analysis.\",\"authors\":\"Soon Yaw Walter Wong, Fen Li Stephanie Ler, Rehena Sultana, Hamid Rahmatullah Bin Abd Razak\",\"doi\":\"10.1186/s43019-022-00166-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Asians have a low venous thromboembolism (VTE) incidence following total knee arthroplasty (TKA). This systematic review and network meta-analysis was conducted to evaluate the best prophylaxis against VTE in Asians following total knee arthroplasty in current literature.</p><p><strong>Materials and methods: </strong>A systematic search of PubMed, Embase and CINAHL was conducted in adherence with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Prophylaxis types were separated into low-molecular-weight heparin (LMWH), novel oral anti-coagulants (NOAC), mechanical-only prophylaxis (MOP) and no prophylaxis (NP). The primary outcome was VTE incidence, grouped according to diagnosis modality (ultrasound, venography, clinical). The secondary outcome was bleeding incidence, grouped into minor and major bleeding.</p><p><strong>Results: </strong>Fourteen eligible articles, totalling 4259 patients, were pooled with the following significant results: NOACs had lower venography-diagnosed VTE incidence than LMWH (12.77%, p = 0.02) and NP (20.64, p < 0.001). MOP had lower venography-diagnosed VTE incidence than LMWH (23.72%, p < 0.001), NOACs (10.95%, p < 0.001) and NP (31.59%, p < 0.001) but, interestingly, a statistically higher ultrasound-diagnosed VTE incidence than LMWH (6.56%, p = 0.024) and NP (4.88%, p = 0.026). No significant differences were observed between prophylaxis types for symptomatic VTE, pulmonary embolism (PE) or death. LMWH and NOACs had a higher minor bleeding incidence than NP (11.71%, p < 0.001 and 6.33%, p < 0.02, respectively). No significant differences were observed between prophylaxis types for major bleeding incidence.</p><p><strong>Conclusion: </strong>NOACs are a superior form of chemoprophylaxis, compared with LMWH, in reducing venography-diagnosed VTE incidence with no added bleeding incidence. However, routine chemoprophylaxis may not be required as LMWH and NOACs do not appear to reduce symptomatic VTE incidence compared with MOP and NP with an increased minor bleeding incidence. Mechanical prophylaxis in the form of graduated compression stockings or intermittent pneumatic compression should be routinely considered with significantly lower rates of venography-diagnosed VTE compared with NP. On the basis of current evidence, we recommend an individualised approach to select the most appropriate prophylaxis type.</p>\",\"PeriodicalId\":4,\"journal\":{\"name\":\"ACS Applied Energy Materials\",\"volume\":\" \",\"pages\":\"37\"},\"PeriodicalIF\":5.5000,\"publicationDate\":\"2022-08-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9375282/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACS Applied Energy Materials\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s43019-022-00166-y\",\"RegionNum\":3,\"RegionCategory\":\"材料科学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CHEMISTRY, PHYSICAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Energy Materials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-022-00166-y","RegionNum":3,"RegionCategory":"材料科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CHEMISTRY, PHYSICAL","Score":null,"Total":0}
What is the best prophylaxis against venous thromboembolism in Asians following total knee arthroplasty? A systematic review and network meta-analysis.
Purpose: Asians have a low venous thromboembolism (VTE) incidence following total knee arthroplasty (TKA). This systematic review and network meta-analysis was conducted to evaluate the best prophylaxis against VTE in Asians following total knee arthroplasty in current literature.
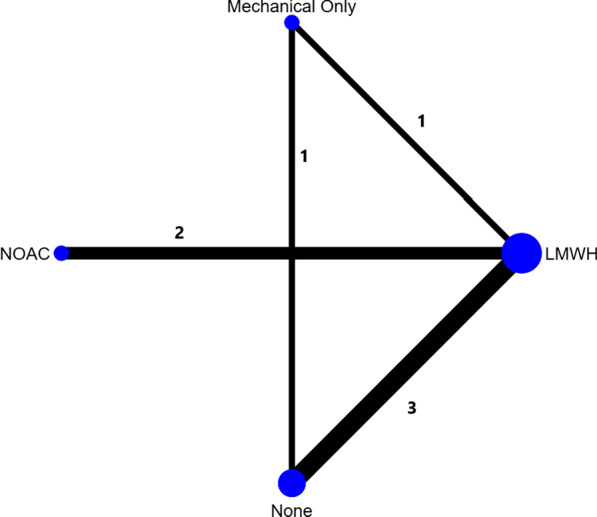
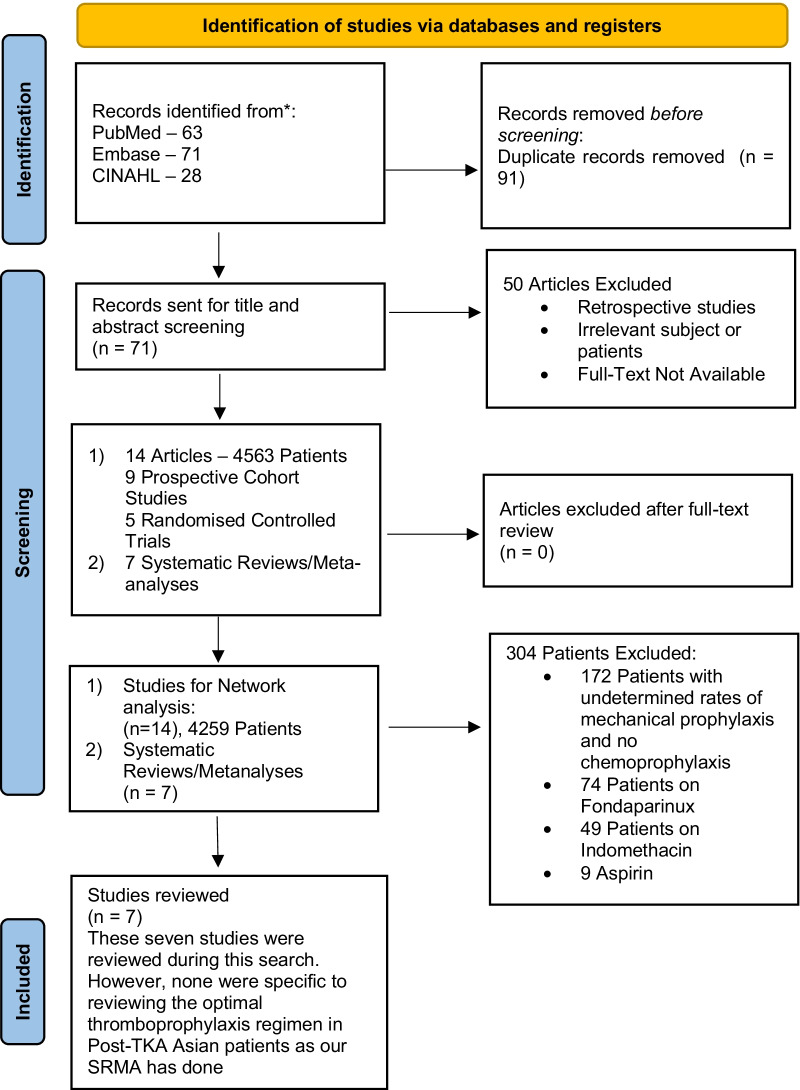
Materials and methods: A systematic search of PubMed, Embase and CINAHL was conducted in adherence with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Prophylaxis types were separated into low-molecular-weight heparin (LMWH), novel oral anti-coagulants (NOAC), mechanical-only prophylaxis (MOP) and no prophylaxis (NP). The primary outcome was VTE incidence, grouped according to diagnosis modality (ultrasound, venography, clinical). The secondary outcome was bleeding incidence, grouped into minor and major bleeding.
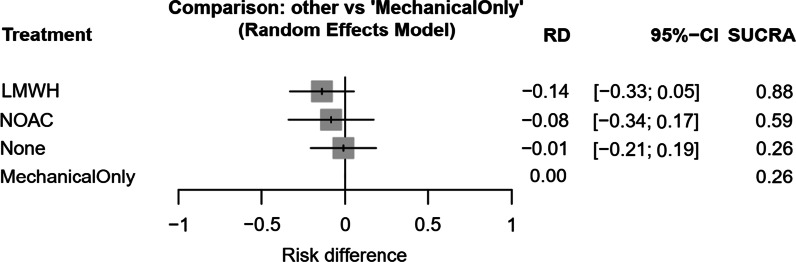
Results: Fourteen eligible articles, totalling 4259 patients, were pooled with the following significant results: NOACs had lower venography-diagnosed VTE incidence than LMWH (12.77%, p = 0.02) and NP (20.64, p < 0.001). MOP had lower venography-diagnosed VTE incidence than LMWH (23.72%, p < 0.001), NOACs (10.95%, p < 0.001) and NP (31.59%, p < 0.001) but, interestingly, a statistically higher ultrasound-diagnosed VTE incidence than LMWH (6.56%, p = 0.024) and NP (4.88%, p = 0.026). No significant differences were observed between prophylaxis types for symptomatic VTE, pulmonary embolism (PE) or death. LMWH and NOACs had a higher minor bleeding incidence than NP (11.71%, p < 0.001 and 6.33%, p < 0.02, respectively). No significant differences were observed between prophylaxis types for major bleeding incidence.
Conclusion: NOACs are a superior form of chemoprophylaxis, compared with LMWH, in reducing venography-diagnosed VTE incidence with no added bleeding incidence. However, routine chemoprophylaxis may not be required as LMWH and NOACs do not appear to reduce symptomatic VTE incidence compared with MOP and NP with an increased minor bleeding incidence. Mechanical prophylaxis in the form of graduated compression stockings or intermittent pneumatic compression should be routinely considered with significantly lower rates of venography-diagnosed VTE compared with NP. On the basis of current evidence, we recommend an individualised approach to select the most appropriate prophylaxis type.
期刊介绍:
ACS Applied Energy Materials is an interdisciplinary journal publishing original research covering all aspects of materials, engineering, chemistry, physics and biology relevant to energy conversion and storage. The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrate knowledge in the areas of materials, engineering, physics, bioscience, and chemistry into important energy applications.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
