{"title":"NRS-2002治疗前营养风险评估预测晚期胆道癌患者预后:一项单中心回顾性研究","authors":"Se Eung Oh, Juong Soon Park, Hei-Cheul Jeung","doi":"10.7762/cnr.2022.11.3.183","DOIUrl":null,"url":null,"abstract":"<p><p>We investigated the predictors of survival in patients with advanced BTC according to their baseline nutritional status estimated by the Nutritional Risk Screening (NRS)-2002. From September 2006 to July 2017, we reviewed the data of 601 inpatients with BTC. Data on demographic and clinical parameters was collected from electronic medical records, and overall survival (OS) and progression-free survival were analyzed using the Kaplan-Meier method and the stepwise Cox regression analysis. Patients with an NRS-2002 score of ≤ 2, 3, and ≥ 4 were respectively classified as \"no risk,\" \"moderate risk,\" \"high risk.\" Following initial NRS-2002 score, 333 patients (55%) were classified as \"no-risk,\" 109 patients (18%) as \"moderate-risk,\" and 159 patients (27%) as \"high-risk.\" Survival analysis demonstrated significant differences in the median OS: \"no-risk\": 12.6 months (95% confidence interval [CI], 11.5-13.7); \"moderate-risk\": 6.1 months (95% CI, 4.3-8.0); and \"high-risk\": 3.9 months (95% CI, 3.2-4.6) (p < 0.001). NRS-2002 score was an independent factor for OS (hazard ratio [HR], 1.616 for \"moderate-risk\", 95% CI, 1.288-2.027, p < 0.001; HR, 2.121 for \"high-risk\", 95% CI, 1.722-2.612, p < 0.001), along with liver metastasis, peritoneal seeding, white blood cell count, platelet count, neutrophil-to-lymphocyte ratio, cholesterol, carcinoembryonic antigen, and carbohydrate antigen 19-9. In conclusion, baseline NRS-2002 is an appropriate method for discriminating those who are already malnourished and who have poor prognosis in advanced BTC patient. Significance of these results merit further validation to be integrated in the routine practice to improve quality of care in BTC patients.</p>","PeriodicalId":72617,"journal":{"name":"Clinical nutrition research","volume":"11 3","pages":"183-193"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b9/e7/cnr-11-183.PMC9348911.pdf","citationCount":"2","resultStr":"{\"title\":\"Pre-treatment Nutritional Risk Assessment by NRS-2002 Predicts Prognosis in Patients With Advanced Biliary Tract Cancer: A Single Center Retrospective Study.\",\"authors\":\"Se Eung Oh, Juong Soon Park, Hei-Cheul Jeung\",\"doi\":\"10.7762/cnr.2022.11.3.183\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We investigated the predictors of survival in patients with advanced BTC according to their baseline nutritional status estimated by the Nutritional Risk Screening (NRS)-2002. From September 2006 to July 2017, we reviewed the data of 601 inpatients with BTC. Data on demographic and clinical parameters was collected from electronic medical records, and overall survival (OS) and progression-free survival were analyzed using the Kaplan-Meier method and the stepwise Cox regression analysis. Patients with an NRS-2002 score of ≤ 2, 3, and ≥ 4 were respectively classified as \\\"no risk,\\\" \\\"moderate risk,\\\" \\\"high risk.\\\" Following initial NRS-2002 score, 333 patients (55%) were classified as \\\"no-risk,\\\" 109 patients (18%) as \\\"moderate-risk,\\\" and 159 patients (27%) as \\\"high-risk.\\\" Survival analysis demonstrated significant differences in the median OS: \\\"no-risk\\\": 12.6 months (95% confidence interval [CI], 11.5-13.7); \\\"moderate-risk\\\": 6.1 months (95% CI, 4.3-8.0); and \\\"high-risk\\\": 3.9 months (95% CI, 3.2-4.6) (p < 0.001). NRS-2002 score was an independent factor for OS (hazard ratio [HR], 1.616 for \\\"moderate-risk\\\", 95% CI, 1.288-2.027, p < 0.001; HR, 2.121 for \\\"high-risk\\\", 95% CI, 1.722-2.612, p < 0.001), along with liver metastasis, peritoneal seeding, white blood cell count, platelet count, neutrophil-to-lymphocyte ratio, cholesterol, carcinoembryonic antigen, and carbohydrate antigen 19-9. In conclusion, baseline NRS-2002 is an appropriate method for discriminating those who are already malnourished and who have poor prognosis in advanced BTC patient. Significance of these results merit further validation to be integrated in the routine practice to improve quality of care in BTC patients.</p>\",\"PeriodicalId\":72617,\"journal\":{\"name\":\"Clinical nutrition research\",\"volume\":\"11 3\",\"pages\":\"183-193\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b9/e7/cnr-11-183.PMC9348911.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical nutrition research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7762/cnr.2022.11.3.183\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical nutrition research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7762/cnr.2022.11.3.183","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Pre-treatment Nutritional Risk Assessment by NRS-2002 Predicts Prognosis in Patients With Advanced Biliary Tract Cancer: A Single Center Retrospective Study.
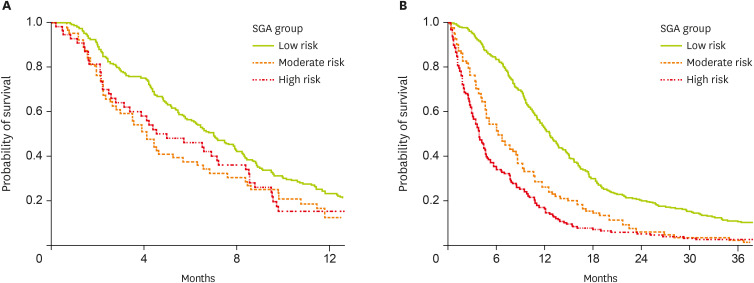
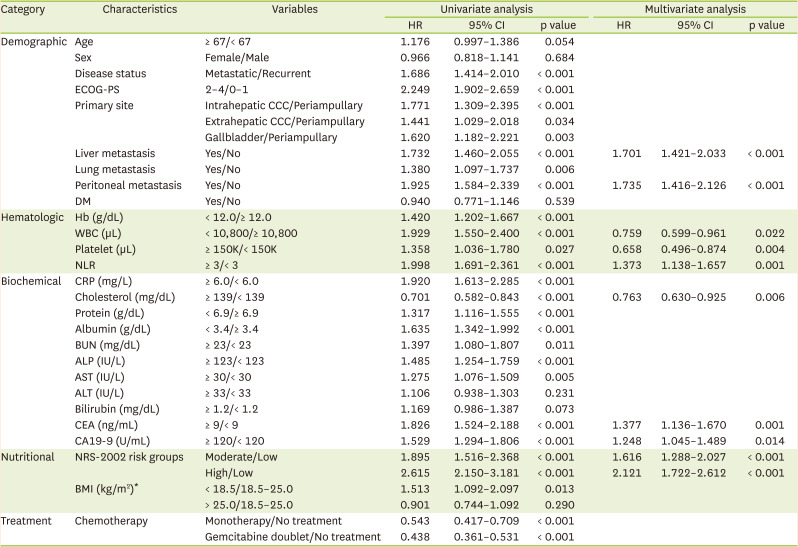
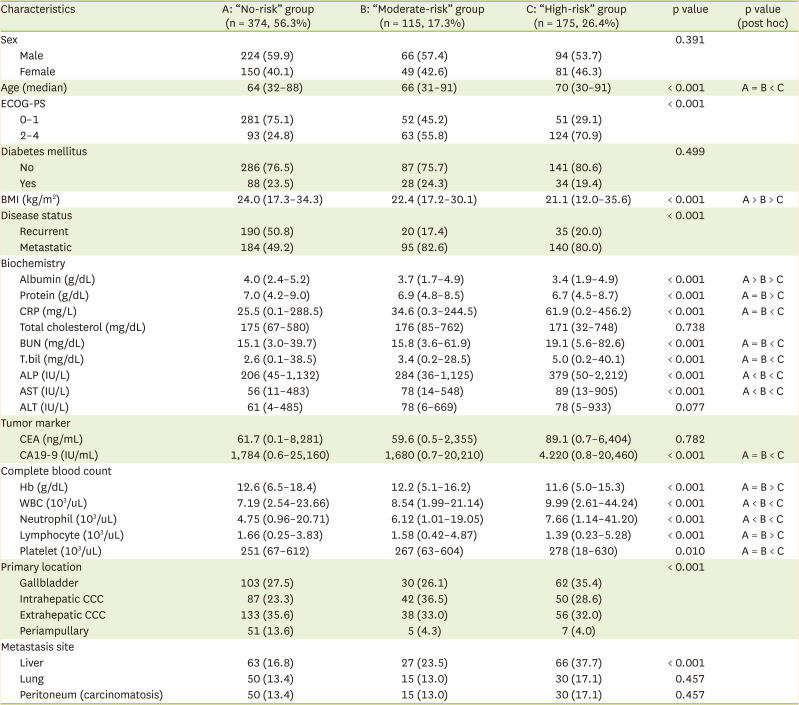
We investigated the predictors of survival in patients with advanced BTC according to their baseline nutritional status estimated by the Nutritional Risk Screening (NRS)-2002. From September 2006 to July 2017, we reviewed the data of 601 inpatients with BTC. Data on demographic and clinical parameters was collected from electronic medical records, and overall survival (OS) and progression-free survival were analyzed using the Kaplan-Meier method and the stepwise Cox regression analysis. Patients with an NRS-2002 score of ≤ 2, 3, and ≥ 4 were respectively classified as "no risk," "moderate risk," "high risk." Following initial NRS-2002 score, 333 patients (55%) were classified as "no-risk," 109 patients (18%) as "moderate-risk," and 159 patients (27%) as "high-risk." Survival analysis demonstrated significant differences in the median OS: "no-risk": 12.6 months (95% confidence interval [CI], 11.5-13.7); "moderate-risk": 6.1 months (95% CI, 4.3-8.0); and "high-risk": 3.9 months (95% CI, 3.2-4.6) (p < 0.001). NRS-2002 score was an independent factor for OS (hazard ratio [HR], 1.616 for "moderate-risk", 95% CI, 1.288-2.027, p < 0.001; HR, 2.121 for "high-risk", 95% CI, 1.722-2.612, p < 0.001), along with liver metastasis, peritoneal seeding, white blood cell count, platelet count, neutrophil-to-lymphocyte ratio, cholesterol, carcinoembryonic antigen, and carbohydrate antigen 19-9. In conclusion, baseline NRS-2002 is an appropriate method for discriminating those who are already malnourished and who have poor prognosis in advanced BTC patient. Significance of these results merit further validation to be integrated in the routine practice to improve quality of care in BTC patients.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
