Clément Javaux, Clémentine Daveau, Clotilde Bettinger, Mathieu Daurade, Céline Dupieux-Chabert, Fabien Craighero, Carine Fuchsmann, Philippe Céruse, Arnaud Gleizal, Nicolas Sigaux, Tristan Ferry, Florent Valour, The Lyon Bji Study Group
{"title":"下颌骨重建后骨皮皮瓣相关骨髓炎:一项新出现的复杂骨感染的队列研究。","authors":"Clément Javaux, Clémentine Daveau, Clotilde Bettinger, Mathieu Daurade, Céline Dupieux-Chabert, Fabien Craighero, Carine Fuchsmann, Philippe Céruse, Arnaud Gleizal, Nicolas Sigaux, Tristan Ferry, Florent Valour, The Lyon Bji Study Group","doi":"10.5194/jbji-7-127-2022","DOIUrl":null,"url":null,"abstract":"<p><p>Osteocutaneous flap (OCF) mandible reconstruction is at high risk for surgical site infection. This study aimed to describe diagnosis, management, and outcome of OCF-related osteomyelitis. All patients managed at our institution for an OCF-related osteomyelitis following mandible reconstruction were included in a retrospective cohort study (2012-2019). Microbiology was described according to gold-standard surgical samples, considering all virulent pathogens, and potential contaminants if present on at least two samples. Determinants of treatment failure were assessed by logistic regression and Kaplan-Meier curve analysis. The 48 included patients (median age 60.5 (IQR, 52.4-66.6) years) benefited from OCF mandible reconstruction mostly for carcinoma ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>27</mn> <mo>/</mo> <mn>48</mn></mrow> </math> ; 56.3 %) or osteoradionecrosis ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>12</mn> <mo>/</mo> <mn>48</mn></mrow> </math> ; 25.0 %). OCF-related osteomyelitis was mostly early ( <math><mrow><mo>≤</mo> <mn>3</mn></mrow> </math> months post-surgery; <math><mrow><mi>n</mi> <mo>=</mo> <mn>43</mn> <mo>/</mo> <mn>48</mn></mrow> </math> ; 89.6 %), presenting with local inflammation ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>28</mn> <mo>/</mo> <mn>47</mn></mrow> </math> ; 59.6 %), nonunion (wound dehiscence) or sinus tract ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>28</mn> <mo>/</mo> <mn>47</mn></mrow> </math> ; 59.6 %), and/or bone or device exposure ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>21</mn> <mo>/</mo> <mn>47</mn></mrow> </math> ; 44.7 %). Main implicated pathogens were Enterobacteriaceae ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>25</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 61.0 %), streptococci ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>22</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 53.7 %), <i>Staphylococcus aureus</i> ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>10</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 24.4 %), enterococci ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>9</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 22.0 %), non-fermenting Gram-negative bacilli ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>8</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 19.5 %), and anaerobes ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>8</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 19.5 %). Thirty-nine patients (81.3 %) benefited from surgery, consisting of debridement with implant retention (DAIR) in <math><mrow><mn>25</mn> <mo>/</mo> <mn>39</mn></mrow> </math> (64.1 %) cases, associated with 93 (IQR, 64-128) days of antimicrobial therapy. After a follow-up of 18 (IQR, 11-31) months, <math><mrow><mn>24</mn> <mo>/</mo> <mn>48</mn></mrow> </math> (50.0 %) treatment failures were observed. Determinants of treatment outcomes were DAIR (OR, 3.333; 95 % CI, 1.020-10.898) and an early infectious disease specialist referral (OR, 0.236 if <math><mrow><mo>≤</mo> <mn>2</mn></mrow> </math> weeks; 95 % CI, 0.062-0.933). OCF-related osteomyelitis following mandibular reconstruction represents difficult-to-treat infections. Our results advocate for a multidisciplinary management, including an early infectious-disease-specialist referral to manage the antimicrobial therapy driven by complex microbiological documentation.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":" ","pages":"127-136"},"PeriodicalIF":2.8000,"publicationDate":"2022-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9285487/pdf/","citationCount":"0","resultStr":"{\"title\":\"Osteocutaneous-flap-related osteomyelitis following mandibular reconstruction: a cohort study of an emerging and complex bone infection.\",\"authors\":\"Clément Javaux, Clémentine Daveau, Clotilde Bettinger, Mathieu Daurade, Céline Dupieux-Chabert, Fabien Craighero, Carine Fuchsmann, Philippe Céruse, Arnaud Gleizal, Nicolas Sigaux, Tristan Ferry, Florent Valour, The Lyon Bji Study Group\",\"doi\":\"10.5194/jbji-7-127-2022\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Osteocutaneous flap (OCF) mandible reconstruction is at high risk for surgical site infection. This study aimed to describe diagnosis, management, and outcome of OCF-related osteomyelitis. All patients managed at our institution for an OCF-related osteomyelitis following mandible reconstruction were included in a retrospective cohort study (2012-2019). Microbiology was described according to gold-standard surgical samples, considering all virulent pathogens, and potential contaminants if present on at least two samples. Determinants of treatment failure were assessed by logistic regression and Kaplan-Meier curve analysis. The 48 included patients (median age 60.5 (IQR, 52.4-66.6) years) benefited from OCF mandible reconstruction mostly for carcinoma ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>27</mn> <mo>/</mo> <mn>48</mn></mrow> </math> ; 56.3 %) or osteoradionecrosis ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>12</mn> <mo>/</mo> <mn>48</mn></mrow> </math> ; 25.0 %). OCF-related osteomyelitis was mostly early ( <math><mrow><mo>≤</mo> <mn>3</mn></mrow> </math> months post-surgery; <math><mrow><mi>n</mi> <mo>=</mo> <mn>43</mn> <mo>/</mo> <mn>48</mn></mrow> </math> ; 89.6 %), presenting with local inflammation ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>28</mn> <mo>/</mo> <mn>47</mn></mrow> </math> ; 59.6 %), nonunion (wound dehiscence) or sinus tract ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>28</mn> <mo>/</mo> <mn>47</mn></mrow> </math> ; 59.6 %), and/or bone or device exposure ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>21</mn> <mo>/</mo> <mn>47</mn></mrow> </math> ; 44.7 %). Main implicated pathogens were Enterobacteriaceae ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>25</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 61.0 %), streptococci ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>22</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 53.7 %), <i>Staphylococcus aureus</i> ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>10</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 24.4 %), enterococci ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>9</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 22.0 %), non-fermenting Gram-negative bacilli ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>8</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 19.5 %), and anaerobes ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>8</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 19.5 %). Thirty-nine patients (81.3 %) benefited from surgery, consisting of debridement with implant retention (DAIR) in <math><mrow><mn>25</mn> <mo>/</mo> <mn>39</mn></mrow> </math> (64.1 %) cases, associated with 93 (IQR, 64-128) days of antimicrobial therapy. After a follow-up of 18 (IQR, 11-31) months, <math><mrow><mn>24</mn> <mo>/</mo> <mn>48</mn></mrow> </math> (50.0 %) treatment failures were observed. Determinants of treatment outcomes were DAIR (OR, 3.333; 95 % CI, 1.020-10.898) and an early infectious disease specialist referral (OR, 0.236 if <math><mrow><mo>≤</mo> <mn>2</mn></mrow> </math> weeks; 95 % CI, 0.062-0.933). OCF-related osteomyelitis following mandibular reconstruction represents difficult-to-treat infections. Our results advocate for a multidisciplinary management, including an early infectious-disease-specialist referral to manage the antimicrobial therapy driven by complex microbiological documentation.</p>\",\"PeriodicalId\":15271,\"journal\":{\"name\":\"Journal of Bone and Joint Infection\",\"volume\":\" \",\"pages\":\"127-136\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2022-06-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9285487/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Bone and Joint Infection\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5194/jbji-7-127-2022\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-7-127-2022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Osteocutaneous-flap-related osteomyelitis following mandibular reconstruction: a cohort study of an emerging and complex bone infection.
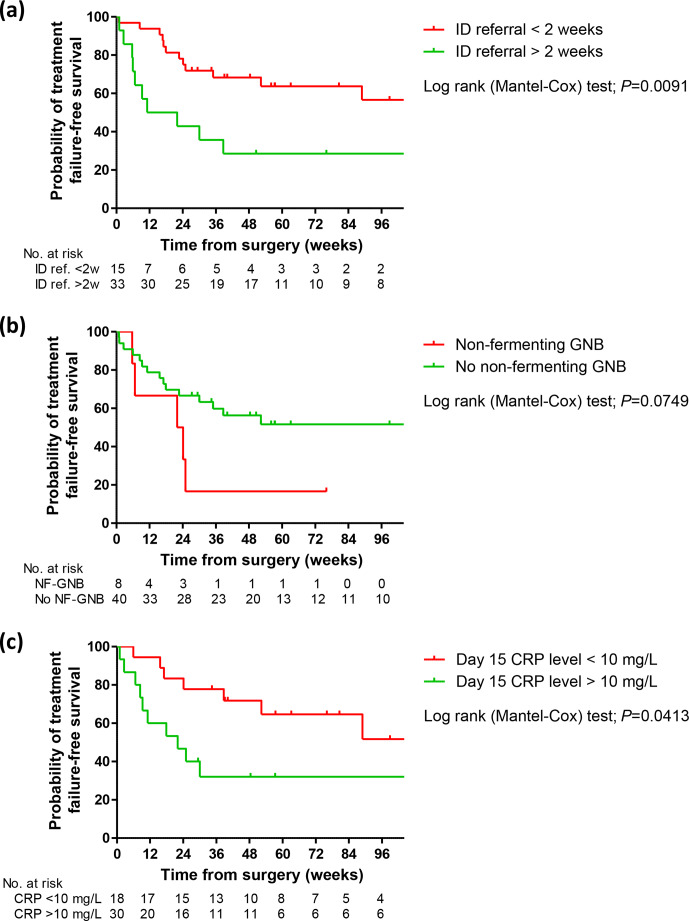
Osteocutaneous flap (OCF) mandible reconstruction is at high risk for surgical site infection. This study aimed to describe diagnosis, management, and outcome of OCF-related osteomyelitis. All patients managed at our institution for an OCF-related osteomyelitis following mandible reconstruction were included in a retrospective cohort study (2012-2019). Microbiology was described according to gold-standard surgical samples, considering all virulent pathogens, and potential contaminants if present on at least two samples. Determinants of treatment failure were assessed by logistic regression and Kaplan-Meier curve analysis. The 48 included patients (median age 60.5 (IQR, 52.4-66.6) years) benefited from OCF mandible reconstruction mostly for carcinoma ( ; 56.3 %) or osteoradionecrosis ( ; 25.0 %). OCF-related osteomyelitis was mostly early ( months post-surgery; ; 89.6 %), presenting with local inflammation ( ; 59.6 %), nonunion (wound dehiscence) or sinus tract ( ; 59.6 %), and/or bone or device exposure ( ; 44.7 %). Main implicated pathogens were Enterobacteriaceae ( ; 61.0 %), streptococci ( ; 53.7 %), Staphylococcus aureus ( ; 24.4 %), enterococci ( ; 22.0 %), non-fermenting Gram-negative bacilli ( ; 19.5 %), and anaerobes ( ; 19.5 %). Thirty-nine patients (81.3 %) benefited from surgery, consisting of debridement with implant retention (DAIR) in (64.1 %) cases, associated with 93 (IQR, 64-128) days of antimicrobial therapy. After a follow-up of 18 (IQR, 11-31) months, (50.0 %) treatment failures were observed. Determinants of treatment outcomes were DAIR (OR, 3.333; 95 % CI, 1.020-10.898) and an early infectious disease specialist referral (OR, 0.236 if weeks; 95 % CI, 0.062-0.933). OCF-related osteomyelitis following mandibular reconstruction represents difficult-to-treat infections. Our results advocate for a multidisciplinary management, including an early infectious-disease-specialist referral to manage the antimicrobial therapy driven by complex microbiological documentation.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
