{"title":"幕状硬脑膜动静脉瘘表现为上颈髓静脉充血性水肿。","authors":"Yuichiro Ohnishi, Tomofumi Takenaka, Sho Fujiwara","doi":"10.2176/jns-nmc.2022-0014","DOIUrl":null,"url":null,"abstract":"<p><p>Tentorial dural arteriovenous fistula (DAVF) is an aggressive vascular lesion causing progressive neurological deficits. Venous congestive cervical edema is a rare phenomenon caused by tentorial DAVF. Obliteration of the fistula and venous drainage should be the goal of treatment. A 62-year-old man was admitted with lower limb weakness and numbness. Magnetic resonance imaging (MRI) revealed extensive edema of the upper cervical cord with signal flow void at the anterior spinal cord. Internal carotid angiography revealed a tentorial arteriovenous shunt near the superior petrosal sinus fed mainly by the tentorial artery. The petrosal vein was dilated, with the transverse pontine vein, medial medullary vein, and anterior spinal vein as the main drainage route. This suggests that venous hypertension triggered the upper cervical cord edema. MRI with gadolinium enhancement showed that the varix was located just distal to the shunt. Microsurgical obliteration of the fistula and venous drainage were achieved via a suboccipital approach. A postoperative evaluation showed the disappearance of the cervical cord edema with improved clinical symptoms. Tentorial DAVF with spinal venous drainage presents with mild and slow progression of symptoms. Differential diagnosis and definite treatment are mandatory to avoid a delayed diagnosis and irreversible symptoms.</p>","PeriodicalId":19260,"journal":{"name":"NMC Case Report Journal","volume":" ","pages":"193-198"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/43/23/2188-4226-9-0193.PMC9256014.pdf","citationCount":"0","resultStr":"{\"title\":\"Tentorial Dural Arteriovenous Fistula Presenting with Venous Congestive Edema of the Upper Cervical Cord.\",\"authors\":\"Yuichiro Ohnishi, Tomofumi Takenaka, Sho Fujiwara\",\"doi\":\"10.2176/jns-nmc.2022-0014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Tentorial dural arteriovenous fistula (DAVF) is an aggressive vascular lesion causing progressive neurological deficits. Venous congestive cervical edema is a rare phenomenon caused by tentorial DAVF. Obliteration of the fistula and venous drainage should be the goal of treatment. A 62-year-old man was admitted with lower limb weakness and numbness. Magnetic resonance imaging (MRI) revealed extensive edema of the upper cervical cord with signal flow void at the anterior spinal cord. Internal carotid angiography revealed a tentorial arteriovenous shunt near the superior petrosal sinus fed mainly by the tentorial artery. The petrosal vein was dilated, with the transverse pontine vein, medial medullary vein, and anterior spinal vein as the main drainage route. This suggests that venous hypertension triggered the upper cervical cord edema. MRI with gadolinium enhancement showed that the varix was located just distal to the shunt. Microsurgical obliteration of the fistula and venous drainage were achieved via a suboccipital approach. A postoperative evaluation showed the disappearance of the cervical cord edema with improved clinical symptoms. Tentorial DAVF with spinal venous drainage presents with mild and slow progression of symptoms. Differential diagnosis and definite treatment are mandatory to avoid a delayed diagnosis and irreversible symptoms.</p>\",\"PeriodicalId\":19260,\"journal\":{\"name\":\"NMC Case Report Journal\",\"volume\":\" \",\"pages\":\"193-198\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-06-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/43/23/2188-4226-9-0193.PMC9256014.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NMC Case Report Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2176/jns-nmc.2022-0014\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC Case Report Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2022-0014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Tentorial Dural Arteriovenous Fistula Presenting with Venous Congestive Edema of the Upper Cervical Cord.
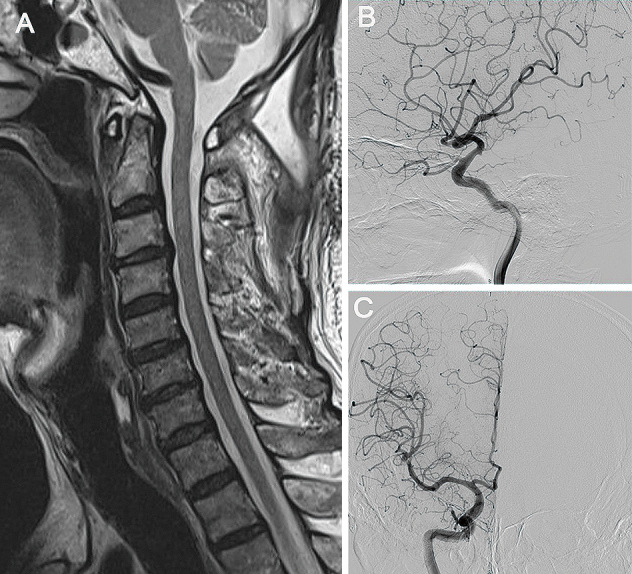
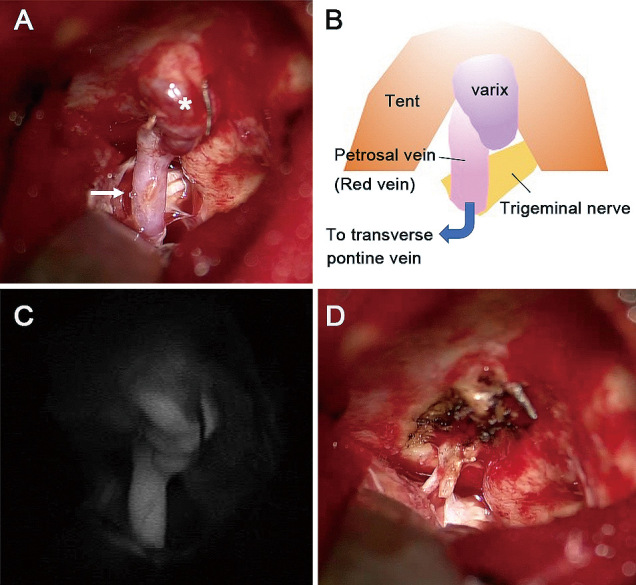
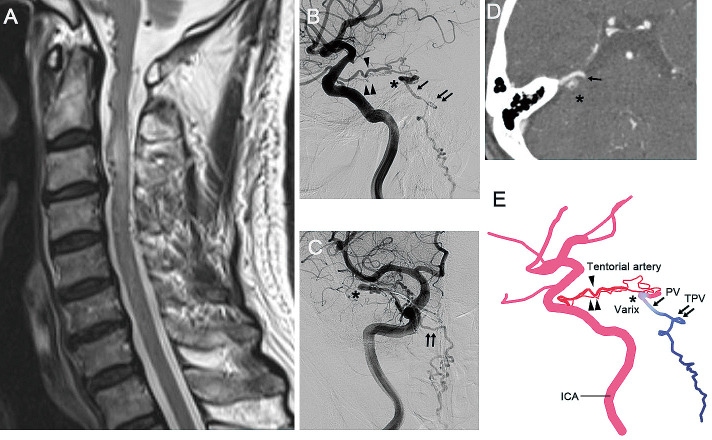
Tentorial dural arteriovenous fistula (DAVF) is an aggressive vascular lesion causing progressive neurological deficits. Venous congestive cervical edema is a rare phenomenon caused by tentorial DAVF. Obliteration of the fistula and venous drainage should be the goal of treatment. A 62-year-old man was admitted with lower limb weakness and numbness. Magnetic resonance imaging (MRI) revealed extensive edema of the upper cervical cord with signal flow void at the anterior spinal cord. Internal carotid angiography revealed a tentorial arteriovenous shunt near the superior petrosal sinus fed mainly by the tentorial artery. The petrosal vein was dilated, with the transverse pontine vein, medial medullary vein, and anterior spinal vein as the main drainage route. This suggests that venous hypertension triggered the upper cervical cord edema. MRI with gadolinium enhancement showed that the varix was located just distal to the shunt. Microsurgical obliteration of the fistula and venous drainage were achieved via a suboccipital approach. A postoperative evaluation showed the disappearance of the cervical cord edema with improved clinical symptoms. Tentorial DAVF with spinal venous drainage presents with mild and slow progression of symptoms. Differential diagnosis and definite treatment are mandatory to avoid a delayed diagnosis and irreversible symptoms.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
