Maja Mijic, Ivona Saric, Bozena Delija, Milos Lalovac, Nikola Sobocan, Eva Radetic, Dora Martincevic, Tajana Filipec Kanizaj
{"title":"PBC 患者移植前评估和肝移植结果","authors":"Maja Mijic, Ivona Saric, Bozena Delija, Milos Lalovac, Nikola Sobocan, Eva Radetic, Dora Martincevic, Tajana Filipec Kanizaj","doi":"10.1155/2022/7831165","DOIUrl":null,"url":null,"abstract":"<p><p>Primary biliary cholangitis (PBC) is an autoimmune chronic cholestatic liver disease characterized by progressive cholangiocyte and bile duct destruction leading to fibrosis and finally to liver cirrhosis. The presence of disease-specific serological antimitochondrial antibody (AMA) together with elevated alkaline phosphatase (ALP) as a biomarker of cholestasis is sufficient for diagnosis. Ursodeoxycholic acid (UDCA) is the first treatment option for PBC. Up to 40% of patients have an incomplete response to therapy, and over time disease progresses to liver cirrhosis. Several risk scores are proposed for better evaluation of patients before and during treatment to stratify patients at increased risk of disease progression. GLOBE score and UK PBC risk score are used for the evaluation of UDCA treatment and Mayo risk score for transplant-free survival. Liver transplantation (LT) is the only treatment option for end-stage liver disease. More than 10 years after LT, 40% of patients experience recurrence of the disease. A liver biopsy is required to establish rPBC (recurrent primary biliary cholangitis). The only treatment option for rPBC is UDCA, and data show biochemical and clinical improvement, plus potential beneficial effects for use after transplantation for the prevention of rPBC development. Additional studies are required to assess the full impact of rPBC on graft and recipient survival and for treatment options for rPBC.</p>","PeriodicalId":48755,"journal":{"name":"Canadian Journal of Gastroenterology and Hepatology","volume":" ","pages":"7831165"},"PeriodicalIF":2.3000,"publicationDate":"2022-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9337972/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pretransplant Evaluation and Liver Transplantation Outcome in PBC Patients.\",\"authors\":\"Maja Mijic, Ivona Saric, Bozena Delija, Milos Lalovac, Nikola Sobocan, Eva Radetic, Dora Martincevic, Tajana Filipec Kanizaj\",\"doi\":\"10.1155/2022/7831165\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Primary biliary cholangitis (PBC) is an autoimmune chronic cholestatic liver disease characterized by progressive cholangiocyte and bile duct destruction leading to fibrosis and finally to liver cirrhosis. The presence of disease-specific serological antimitochondrial antibody (AMA) together with elevated alkaline phosphatase (ALP) as a biomarker of cholestasis is sufficient for diagnosis. Ursodeoxycholic acid (UDCA) is the first treatment option for PBC. Up to 40% of patients have an incomplete response to therapy, and over time disease progresses to liver cirrhosis. Several risk scores are proposed for better evaluation of patients before and during treatment to stratify patients at increased risk of disease progression. GLOBE score and UK PBC risk score are used for the evaluation of UDCA treatment and Mayo risk score for transplant-free survival. Liver transplantation (LT) is the only treatment option for end-stage liver disease. More than 10 years after LT, 40% of patients experience recurrence of the disease. A liver biopsy is required to establish rPBC (recurrent primary biliary cholangitis). The only treatment option for rPBC is UDCA, and data show biochemical and clinical improvement, plus potential beneficial effects for use after transplantation for the prevention of rPBC development. Additional studies are required to assess the full impact of rPBC on graft and recipient survival and for treatment options for rPBC.</p>\",\"PeriodicalId\":48755,\"journal\":{\"name\":\"Canadian Journal of Gastroenterology and Hepatology\",\"volume\":\" \",\"pages\":\"7831165\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2022-07-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9337972/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Gastroenterology and Hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/7831165\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2022/7831165","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Pretransplant Evaluation and Liver Transplantation Outcome in PBC Patients.
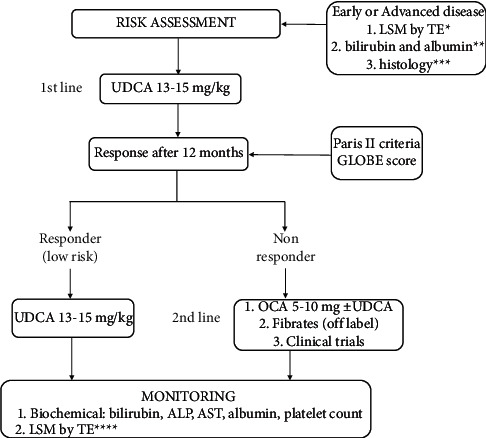
Primary biliary cholangitis (PBC) is an autoimmune chronic cholestatic liver disease characterized by progressive cholangiocyte and bile duct destruction leading to fibrosis and finally to liver cirrhosis. The presence of disease-specific serological antimitochondrial antibody (AMA) together with elevated alkaline phosphatase (ALP) as a biomarker of cholestasis is sufficient for diagnosis. Ursodeoxycholic acid (UDCA) is the first treatment option for PBC. Up to 40% of patients have an incomplete response to therapy, and over time disease progresses to liver cirrhosis. Several risk scores are proposed for better evaluation of patients before and during treatment to stratify patients at increased risk of disease progression. GLOBE score and UK PBC risk score are used for the evaluation of UDCA treatment and Mayo risk score for transplant-free survival. Liver transplantation (LT) is the only treatment option for end-stage liver disease. More than 10 years after LT, 40% of patients experience recurrence of the disease. A liver biopsy is required to establish rPBC (recurrent primary biliary cholangitis). The only treatment option for rPBC is UDCA, and data show biochemical and clinical improvement, plus potential beneficial effects for use after transplantation for the prevention of rPBC development. Additional studies are required to assess the full impact of rPBC on graft and recipient survival and for treatment options for rPBC.
期刊介绍:
Canadian Journal of Gastroenterology and Hepatology is a peer-reviewed, open access journal that publishes original research articles, review articles, and clinical studies in all areas of gastroenterology and liver disease - medicine and surgery.
The Canadian Journal of Gastroenterology and Hepatology is sponsored by the Canadian Association of Gastroenterology and the Canadian Association for the Study of the Liver.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
