Albert Selva-O'Callaghan, Ernesto Trallero-Araguás, Javier Ros, Albert Gil-Vila, Julia Lostes, Antonia Agustí, Judit Riera-Arnau, Marcelo Alvarado-Cárdenas, Iago Pinal-Fernandez
{"title":"癌症相关性肌炎的治疗。","authors":"Albert Selva-O'Callaghan, Ernesto Trallero-Araguás, Javier Ros, Albert Gil-Vila, Julia Lostes, Antonia Agustí, Judit Riera-Arnau, Marcelo Alvarado-Cárdenas, Iago Pinal-Fernandez","doi":"10.1007/s40674-022-00197-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of the review: </strong>Cancer-associated myositis (CAM) is defined as when cancer appears within 3 years of myositis onset. Dermatomyositis and seronegative immune-mediated necrotizing myopathy are the phenotypes mostly related to cancer. In general, treatment principles in myositis patients with and without CAM are similar. However, some aspects of myositis management are particular to CAM, including (a) the need for a multidisciplinary approach and a close relationship with the oncologist, (b) the presence of immunosuppressive and antineoplastic drug interactions, and (c) the role of the long-term immunosuppressive therapy as a risk factor for cancer relapse or development of a second neoplasm. In this review, we will also discuss immunotherapy in patients treated with checkpoint inhibitors as a treatment for their cancer.</p><p><strong>Recent findings: </strong>Studies on cancer risk in patients treated with long-term immunosuppressive drugs, in autoimmune diseases such as systemic lupus erythematosus or rheumatoid arthritis, and in solid organ transplant recipients have shed some light on this topic. Immunotherapy, which has been a great advance for the treatment of some types of malignancy, may be also of interest in CAM, given the special relationship between both disorders.</p><p><strong>Summary: </strong>Management of CAM is a challenge. In this complex scenario, therapeutic decisions must consider both diseases simultaneously.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1007/s40674-022-00197-2.</p>","PeriodicalId":11096,"journal":{"name":"Current Treatment Options in Rheumatology","volume":"8 4","pages":"91-104"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9589595/pdf/","citationCount":"2","resultStr":"{\"title\":\"Management of Cancer-Associated Myositis.\",\"authors\":\"Albert Selva-O'Callaghan, Ernesto Trallero-Araguás, Javier Ros, Albert Gil-Vila, Julia Lostes, Antonia Agustí, Judit Riera-Arnau, Marcelo Alvarado-Cárdenas, Iago Pinal-Fernandez\",\"doi\":\"10.1007/s40674-022-00197-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose of the review: </strong>Cancer-associated myositis (CAM) is defined as when cancer appears within 3 years of myositis onset. Dermatomyositis and seronegative immune-mediated necrotizing myopathy are the phenotypes mostly related to cancer. In general, treatment principles in myositis patients with and without CAM are similar. However, some aspects of myositis management are particular to CAM, including (a) the need for a multidisciplinary approach and a close relationship with the oncologist, (b) the presence of immunosuppressive and antineoplastic drug interactions, and (c) the role of the long-term immunosuppressive therapy as a risk factor for cancer relapse or development of a second neoplasm. In this review, we will also discuss immunotherapy in patients treated with checkpoint inhibitors as a treatment for their cancer.</p><p><strong>Recent findings: </strong>Studies on cancer risk in patients treated with long-term immunosuppressive drugs, in autoimmune diseases such as systemic lupus erythematosus or rheumatoid arthritis, and in solid organ transplant recipients have shed some light on this topic. Immunotherapy, which has been a great advance for the treatment of some types of malignancy, may be also of interest in CAM, given the special relationship between both disorders.</p><p><strong>Summary: </strong>Management of CAM is a challenge. In this complex scenario, therapeutic decisions must consider both diseases simultaneously.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1007/s40674-022-00197-2.</p>\",\"PeriodicalId\":11096,\"journal\":{\"name\":\"Current Treatment Options in Rheumatology\",\"volume\":\"8 4\",\"pages\":\"91-104\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9589595/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Treatment Options in Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40674-022-00197-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Treatment Options in Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40674-022-00197-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
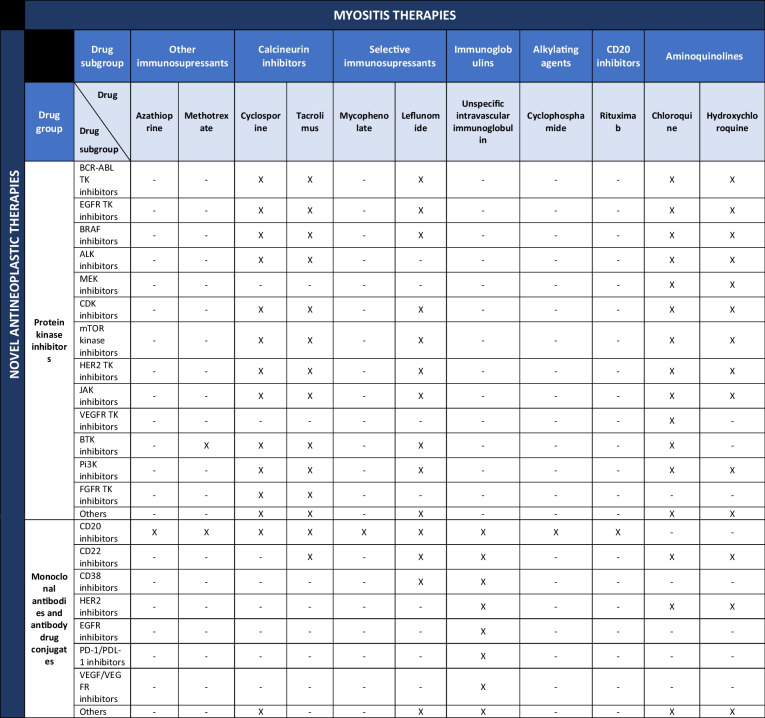
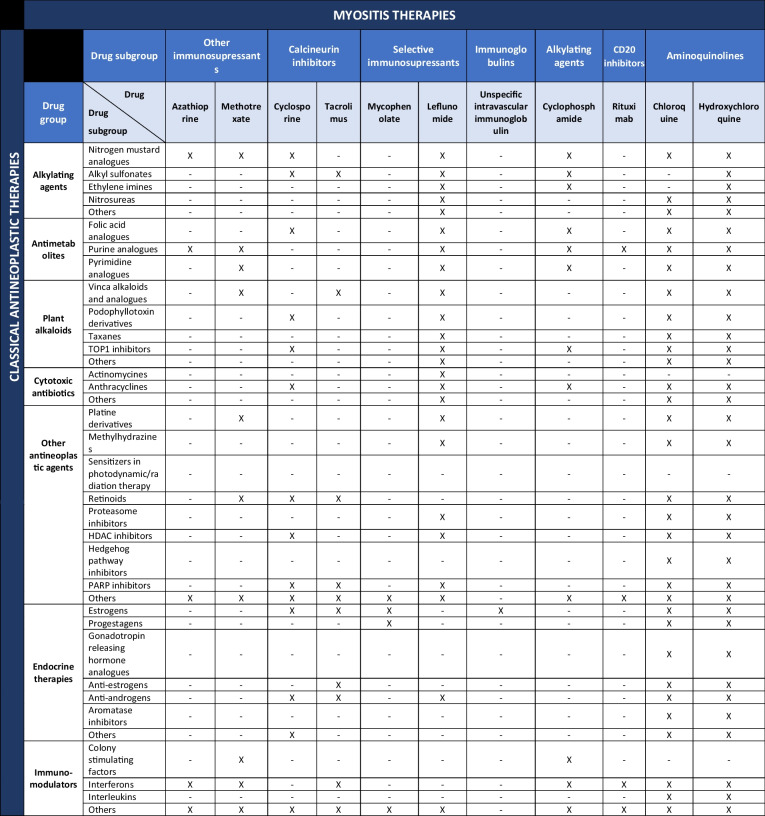
Purpose of the review: Cancer-associated myositis (CAM) is defined as when cancer appears within 3 years of myositis onset. Dermatomyositis and seronegative immune-mediated necrotizing myopathy are the phenotypes mostly related to cancer. In general, treatment principles in myositis patients with and without CAM are similar. However, some aspects of myositis management are particular to CAM, including (a) the need for a multidisciplinary approach and a close relationship with the oncologist, (b) the presence of immunosuppressive and antineoplastic drug interactions, and (c) the role of the long-term immunosuppressive therapy as a risk factor for cancer relapse or development of a second neoplasm. In this review, we will also discuss immunotherapy in patients treated with checkpoint inhibitors as a treatment for their cancer.
Recent findings: Studies on cancer risk in patients treated with long-term immunosuppressive drugs, in autoimmune diseases such as systemic lupus erythematosus or rheumatoid arthritis, and in solid organ transplant recipients have shed some light on this topic. Immunotherapy, which has been a great advance for the treatment of some types of malignancy, may be also of interest in CAM, given the special relationship between both disorders.
Summary: Management of CAM is a challenge. In this complex scenario, therapeutic decisions must consider both diseases simultaneously.
Supplementary information: The online version contains supplementary material available at 10.1007/s40674-022-00197-2.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
