{"title":"经皮二尖瓣合拢切开术和二尖瓣置换术后严重风湿性二尖瓣狭窄的长期预后:10年经验。","authors":"Wasinee Promratpan, Nonthikorn Theerasuwipakorn, Vorarit Lertsuwunseri, Suphot Srimahachota","doi":"10.34172/jcvtr.2022.16","DOIUrl":null,"url":null,"abstract":"<p><p><b><i>Introduction:</i></b> Percutaneous mitral commissurotomy (PTMC) and mitral valve replacement (MVR) are treatments of choice for severe rheumatic mitral stenosis (MS). Data regarding the long-term outcomes of patients who underwent PTMC and MVR are limited. <b><i>Methods:</i></b> A retrospective cohort study was conducted to evaluate the long-term outcomes of patients with severe rheumatic MS who underwent PTMC or MVR between 2010 to 2020. The primary outcome comprised of all-cause death, stroke or systemic embolism, heart failure hospitalization and re-intervention. Cox regression was used to investigate predictors of the primary outcome. <b><i>Results:</i></b> 264 patients were included in analysis, 164 patients (62.1%) in PTMC group and 100 patients in MVR group (37.9%). The majority were females (80.7%) and had atrial fibrillation (68.6%). The mean age was 49.52 (SD: 13.03) years old. MVR group had more age and AF, higher Wilkins' score with smaller MVA. Primary outcome occurred significantly higher in PTMC group (37.2% vs 22%, <i>P</i>=0.002), as well as, re-intervention (18.3% vs 0%, <i>P</i><0.001). However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different. In multivariate Cox regression analysis, PTMC (HR 1.94; 95%CI 1.14, 3.32; <i>P</i>=0.015), older age (HR 1.03; 95%CI 1.01, 1.06; <i>P</i>=0.009) and SPAP > 50 mmHg (HR 2.99; 95%CI 1.01, 8.84; <i>P</i>=0.047) were the only predictors of primary outcome. <b><i>Conclusion:</i></b> Primary outcome occurred in PTMC group more than MVR group which was driven by re-intervention. However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different.</p>","PeriodicalId":15207,"journal":{"name":"Journal of Cardiovascular and Thoracic Research","volume":"14 2","pages":"101-107"},"PeriodicalIF":0.7000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9339733/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-term outcomes of severe rheumatic mitral stenosis after undergoing percutaneous mitral commissurotomy and mitral valve replacement: A 10-year experience.\",\"authors\":\"Wasinee Promratpan, Nonthikorn Theerasuwipakorn, Vorarit Lertsuwunseri, Suphot Srimahachota\",\"doi\":\"10.34172/jcvtr.2022.16\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b><i>Introduction:</i></b> Percutaneous mitral commissurotomy (PTMC) and mitral valve replacement (MVR) are treatments of choice for severe rheumatic mitral stenosis (MS). Data regarding the long-term outcomes of patients who underwent PTMC and MVR are limited. <b><i>Methods:</i></b> A retrospective cohort study was conducted to evaluate the long-term outcomes of patients with severe rheumatic MS who underwent PTMC or MVR between 2010 to 2020. The primary outcome comprised of all-cause death, stroke or systemic embolism, heart failure hospitalization and re-intervention. Cox regression was used to investigate predictors of the primary outcome. <b><i>Results:</i></b> 264 patients were included in analysis, 164 patients (62.1%) in PTMC group and 100 patients in MVR group (37.9%). The majority were females (80.7%) and had atrial fibrillation (68.6%). The mean age was 49.52 (SD: 13.03) years old. MVR group had more age and AF, higher Wilkins' score with smaller MVA. Primary outcome occurred significantly higher in PTMC group (37.2% vs 22%, <i>P</i>=0.002), as well as, re-intervention (18.3% vs 0%, <i>P</i><0.001). However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different. In multivariate Cox regression analysis, PTMC (HR 1.94; 95%CI 1.14, 3.32; <i>P</i>=0.015), older age (HR 1.03; 95%CI 1.01, 1.06; <i>P</i>=0.009) and SPAP > 50 mmHg (HR 2.99; 95%CI 1.01, 8.84; <i>P</i>=0.047) were the only predictors of primary outcome. <b><i>Conclusion:</i></b> Primary outcome occurred in PTMC group more than MVR group which was driven by re-intervention. However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different.</p>\",\"PeriodicalId\":15207,\"journal\":{\"name\":\"Journal of Cardiovascular and Thoracic Research\",\"volume\":\"14 2\",\"pages\":\"101-107\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9339733/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular and Thoracic Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.34172/jcvtr.2022.16\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/6/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular and Thoracic Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34172/jcvtr.2022.16","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/6/12 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
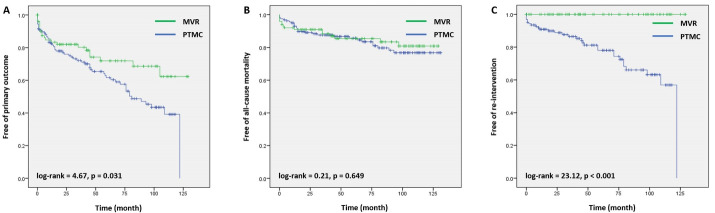
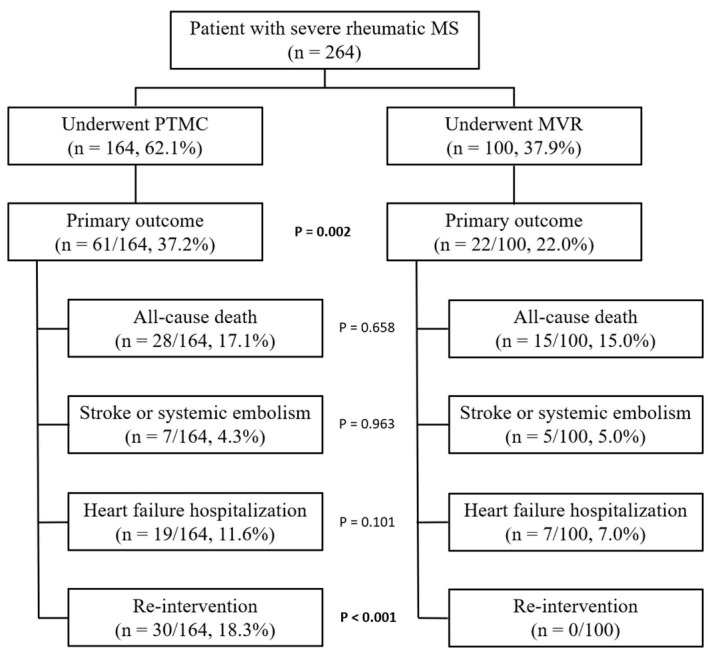
简介:经皮二尖瓣合并术(PTMC)和二尖瓣置换术(MVR)是治疗严重风湿性二尖瓣狭窄(MS)的首选方法。关于PTMC和MVR患者长期预后的数据有限。方法:回顾性队列研究评估2010年至2020年期间接受PTMC或MVR治疗的重度风湿性MS患者的长期预后。主要结局包括全因死亡、中风或全身性栓塞、心力衰竭住院和再干预。采用Cox回归分析主要结局的预测因素。结果:264例患者纳入分析,PTMC组164例(62.1%),MVR组100例(37.9%)。其中以女性居多(80.7%),并伴有心房颤动(68.6%)。平均年龄49.52岁(SD: 13.03)。MVR组年龄和房颤较大,Wilkins评分较高,MVA较小。PTMC组的主要转转率(37.2% vs 22%, P=0.002)、再干预(18.3% vs 0%, PP=0.015)、老年(HR 1.03;95%ci 1.01, 1.06;P=0.009), SPAP > 50 mmHg (HR 2.99;95%ci 1.01, 8.84;P=0.047)是主要结局的唯一预测因子。结论:PTMC组主要转归率高于MVR组,主要转归率由再干预驱动。然而,全因死亡率、中风或全身性栓塞和心力衰竭住院没有显著差异。
Long-term outcomes of severe rheumatic mitral stenosis after undergoing percutaneous mitral commissurotomy and mitral valve replacement: A 10-year experience.
Introduction: Percutaneous mitral commissurotomy (PTMC) and mitral valve replacement (MVR) are treatments of choice for severe rheumatic mitral stenosis (MS). Data regarding the long-term outcomes of patients who underwent PTMC and MVR are limited. Methods: A retrospective cohort study was conducted to evaluate the long-term outcomes of patients with severe rheumatic MS who underwent PTMC or MVR between 2010 to 2020. The primary outcome comprised of all-cause death, stroke or systemic embolism, heart failure hospitalization and re-intervention. Cox regression was used to investigate predictors of the primary outcome. Results: 264 patients were included in analysis, 164 patients (62.1%) in PTMC group and 100 patients in MVR group (37.9%). The majority were females (80.7%) and had atrial fibrillation (68.6%). The mean age was 49.52 (SD: 13.03) years old. MVR group had more age and AF, higher Wilkins' score with smaller MVA. Primary outcome occurred significantly higher in PTMC group (37.2% vs 22%, P=0.002), as well as, re-intervention (18.3% vs 0%, P<0.001). However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different. In multivariate Cox regression analysis, PTMC (HR 1.94; 95%CI 1.14, 3.32; P=0.015), older age (HR 1.03; 95%CI 1.01, 1.06; P=0.009) and SPAP > 50 mmHg (HR 2.99; 95%CI 1.01, 8.84; P=0.047) were the only predictors of primary outcome. Conclusion: Primary outcome occurred in PTMC group more than MVR group which was driven by re-intervention. However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
